Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Is Thoracic Facet & Costovertebral Joint Dysfunction?
The thoracic spine has two distinct joint systems that are often overlooked in standard assessments.
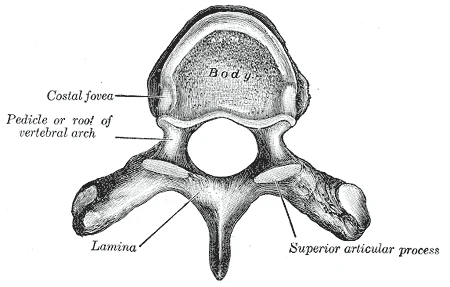
Thoracic facet joints are paired synovial joints at each spinal level, linking the vertebrae posteriorly. They are similar in structure to the more frequently discussed lumbar facet joints, but oriented differently — the thoracic facets sit in a more coronal plane, resisting rotation and extension. Their capsules are richly innervated and capable of producing significant local and referred pain.
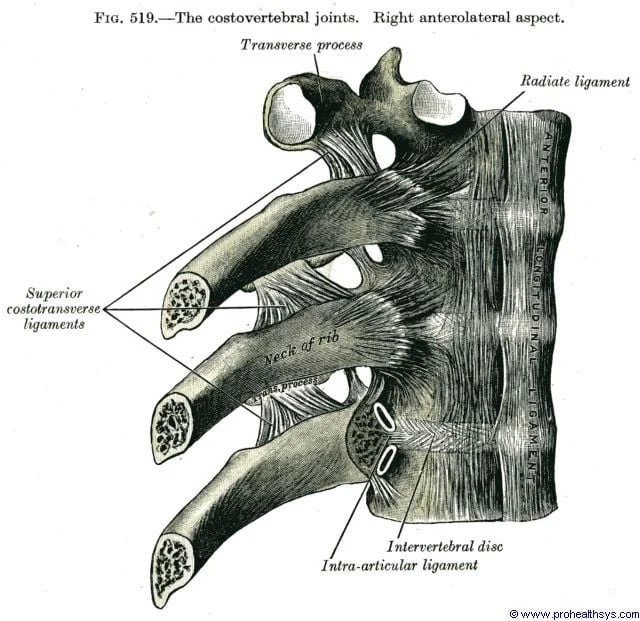
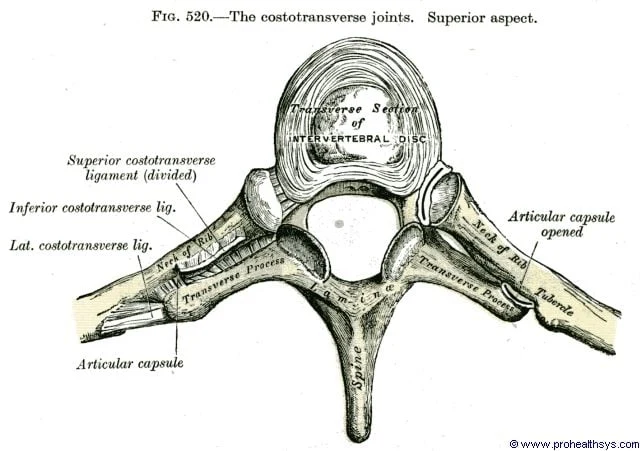
Costovertebral and costotransverse joints connect the ribs to the thoracic spine. Each rib has two articulations: the costovertebral joint (rib head meeting the vertebral body) and the costotransverse joint (rib tubercle meeting the transverse process). These are small synovial joints enclosed in fibrous capsules and embedded within the fascial envelope of the paraspinal region. They are essential for rib cage movement during breathing, rotation, and loading — and they are capable of producing pain referral patterns that are frequently mistaken for visceral, cardiac, or pulmonary conditions.
| Feature | Detail |
|---|---|
| Joints involved | Thoracic facets, costovertebral joints, costotransverse joints |
| Innervation | Medial and lateral branches of dorsal rami; costovertebral joints contain substance P and CGRP-reactive nerve fibres |
| Common levels | T3–T7 (desk worker posture); T1–T4 (overhead/upper limb load); T9–T12 (rotation-dominant sport) |
| Symptom character | Deep, dull ache; often segmental; may refer anteriorly around the chest wall |
| Provocation | Thoracic rotation, sustained flexion, deep breath, direct palpation over costotransverse joint |
| Prevalence of facet pain in chronic thoracic pain | Estimated 34–48% using controlled diagnostic blocks |
Who Typically Experiences This?
Desk Workers and Remote Professionals
Sustained thoracic flexion — the working posture of most desk-based workers — progressively loads the posterior thoracic joints. Over hours at a screen, the thoracic spine settles into kyphosis, the facet joints are approximated posteriorly, and the costovertebral joints lose the mechanical stimulus of thoracic extension and rotation. The result is progressive stiffness, pericostal tension, and a gradual build-up of sensitivity in the paraspinal region that many people describe as "knots" or "tension" between the shoulder blades. This population also commonly experiences referral to the anterior chest that can trigger cardiac concern.
Gym Athletes and Weightlifters
The front rack position in Olympic lifting, overhead pressing, and heavy barbell rowing all place specific demands on thoracic extension mobility and costovertebral joint mechanics. An athlete who lacks adequate thoracic extension will compensate at adjacent segments — often the cervicothoracic junction or lumbar spine — loading those structures instead. Conversely, high-volume loading in thoracic flexion (repeated rowing, deadlifts, bent-over positions) can sensitise the posterior thoracic joints over a training cycle.
Yoga and Pilates Practitioners
Thoracic extension is often emphasised in yoga and pilates practice, and this is generally beneficial. However, practitioners who force thoracic extension without adequate segmental mobility can create shear at specific costovertebral levels — particularly mid-thoracic — rather than achieving the distributed extension the movement requires. This is more common in hypermobile individuals who achieve apparent thoracic range through a few hypermobile segments rather than even distribution.
People Who Have Had Rib Injuries
Prior rib fractures, contusions, or significant respiratory illness involving prolonged, forceful coughing can alter the mechanics of the costovertebral and costotransverse joints. These joints bear significant load during coughing and sneezing, and a history of thoracic cage trauma frequently leaves altered mechanics at the rib-spine interface that persists well beyond tissue healing.
The Fascial Lens: Why We See This Differently
The thoracic spine sits at the convergence of several fascial systems. The posterior thoracic fascia — continuous with the thoracolumbar fascia (TLF) below — envelops the paraspinal compartment and invests the costovertebral joints within a dense fascial sleeve. The intercostal fasciae form compartments between each pair of ribs, containing the intercostal muscles, nerves, and vessels. The paraspinal retinacular sheath described by Willard and colleagues encloses the erector spinae and multifidus in a pressurised compartment that connects the thoracic and lumbar regions as a functional unit.
The costovertebral and costotransverse joints are not free-floating within this system — they are embedded in it. When the posterior thoracic fascia becomes restricted through sustained postural loading, paraspinal compartment pressure increases and the mechanical environment of these joints changes. The joint capsules, which contain substance P and calcitonin gene-related peptide (CGRP) — neuropeptides associated with pain and neurogenic inflammation — become sensitised within this altered fascial context. [1]
This explains a pattern we see regularly in clinical practice: patients with mid-thoracic stiffness and a vague anterior chest ache whose cardiac and pulmonary workup is entirely normal. The pain referral from costovertebral dysfunction follows the intercostal nerve distribution, which runs from the posterior costovertebral joint anteriorly to the sternum. The joint irritation is posterior; the symptoms are anterior. This is not referred pain in the loose sense — it is anatomically predictable, and well documented. [2, 3]
A note on T4 syndrome: In the manual therapy literature, a specific pattern is sometimes described as T4 syndrome — characterised by diffuse upper limb paraesthesia (often bilateral, glove distribution), posterior mid-thoracic pain, and occasionally headache, thought to arise from segmental hypomobility at T4. The mechanism is not fully established, but the clinical pattern is recognisable and responds well to thoracic mobilisation and soft tissue work at the mid-thoracic segment. We encounter this presentation periodically and assess the T4 region specifically when diffuse arm symptoms accompany mid-back stiffness without a clear cervical or peripheral nerve explanation.
What Does the Research Say?
Costovertebral and costotransverse joints are capable of producing significant pain referral to the anterior chest. A provocation study by Young and colleagues (2008) — the only published study of its kind — mapped pain referral patterns from fluoroscopically guided intra-articular injections into asymptomatic costotransverse joints. Pain was described as a deep, dull ache located near the injected joint, with cranio-caudal referral around the rib to the anterior chest in multiple subjects. This establishes the costotransverse joint as a credible source of anterior chest pain in the absence of cardiac or pulmonary pathology. [2]
These joints are richly innervated and capable of neurogenic sensitisation. Immunocytochemical analysis of human costovertebral complexes (Erwin, Jackson & Homonko, 2000) identified substance P and CGRP-reactive nerve fibres within the joint capsule, synovial tissue, and intra-articular meniscoid inclusions — the same neuropeptides associated with pain sensitisation and neurogenic inflammation. This provides the neuroanatomical basis for costovertebral joint pain and its characteristic pseudo-anginal referral patterns. [1]
Costovertebral joint dysfunction is a documented but frequently missed cause of atypical chest pain. A clinical case series from Geneva University Hospital (Arroyo, Jolliet & Junod, 1992) described five patients with atypical chest pain arising from costovertebral dysfunction who had each undergone extensive cardiac and pulmonary investigation before the musculoskeletal diagnosis was made. All cases responded to manual assessment and simple therapeutic manoeuvres. The authors argued that awareness of this condition could reduce unnecessary invasive investigation — an argument that remains as relevant today as it was three decades ago. [3]
How We Approach Thoracic Facet & Costovertebral Dysfunction
Our assessment of the thoracic spine examines the facet joints, costovertebral and costotransverse articulations, and the surrounding fascial environment — including the paraspinal compartment, intercostal fasciae, and the transition zones at the cervicothoracic and thoracolumbar junctions.
Movement assessment looks at segmental thoracic rotation, extension, and rib cage expansion — identifying where restriction is concentrated and where the spine is compensating. Palpation maps the posterior thoracic fascial tension and identifies sensitive costovertebral and costotransverse levels.
Fascial Manipulation is directed at the centres of coordination within the posterior thoracic and intercostal fascial layers where densification is identified. Thoracic joint mobilisation addresses specific segmental restrictions at the facet and costovertebral levels. Movement retraining addresses the postural and loading patterns — thoracic flexion under load, lack of thoracic rotation in daily activity — that drive the mechanical environment producing the problem.
The goal is to restore the mobility and mechanical environment of the thoracic cage so that the joints and fascial structures can distribute load appropriately, rather than concentrating it at sensitised segments.
New to Fascial Manipulation? Read how it works → · How chiropractic adjustments work →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Anterior chest pain should always be evaluated medically to exclude cardiac and pulmonary causes before a musculoskeletal diagnosis is attributed. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Add thoracic extension to your daily routine.
Thoracic extension over a foam roller — positioned horizontally across the mid-back at the level of the stiffness, with hands behind the head for support — is one of the most effective self-mobilisation strategies for mid-thoracic restriction. Move through 3–4 levels over the thoracic spine, spending 30–60 seconds at each. This directly addresses the extension deficit created by sustained desk posture.
2. Incorporate thoracic rotation into movement breaks.
Thoracic rotation — seated or standing, with hands across the chest or reaching overhead — provides mechanical stimulus to the costotransverse joints and paraspinal fascial layers. Two or three minutes of controlled rotation every hour of desk work is a practical and evidence-consistent strategy for reducing cumulative posterior thoracic loading.
3. Reassess your seated position.
Most thoracic stiffness in desk workers is driven by sustained posture, not a single incident. A seat height that allows the hips to be slightly higher than the knees, a screen at eye level, and a keyboard position that keeps the elbows at 90° reduces the anterior thoracic load that produces progressive posterior joint approximation.
4. Don't ignore anterior chest symptoms.
If you are experiencing anterior chest pain — especially if it is new, sharp, or associated with shortness of breath, palpitations, or pain radiating to the arm or jaw — seek medical evaluation to exclude cardiac causes before attributing symptoms to a musculoskeletal source. Once cardiac causes are excluded, musculoskeletal assessment of the posterior thoracic spine is a clinically appropriate next step.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
The thoracolumbar fascia connects the thoracic spine directly to the lumbar region and pelvis — dysfunction at thoracic facet and costovertebral joints often reflects altered load transfer through this shared fascial system. This pillar article explains the TLF and sling mechanics relevant to thoracolumbar pain.
Read Article →Thoracic joint manipulation is one of the best-evidenced manual interventions, producing measurable hypoalgesia, improved motor control, and autonomic effects that extend beyond the treated segment. This article explains the full neurophysiological mechanism behind these regional and remote effects.
Read Article →References
- PubMed Erwin WM, Jackson PC, Homonko DA (2000). Innervation of the human costovertebral joint: implications for clinical back pain syndromes. Journal of Manipulative and Physiological Therapeutics, 23(6), 395–403.
- PubMed Young BA, Gill HE, Wainner RS, Flynn TW (2008). Thoracic costotransverse joint pain patterns: a study in normal volunteers. BMC Musculoskeletal Disorders, 9, 140.
- PubMed Arroyo JF, Jolliet P, Junod AF (1992). Costovertebral joint dysfunction: another misdiagnosed cause of atypical chest pain. Postgraduate Medical Journal, 68(802), 655–659.