 By Dr Steven Hewitt — Chiropractor · AHPRA: CHI0001115420 · 23 May 2026 · ~7 min read
By Dr Steven Hewitt — Chiropractor · AHPRA: CHI0001115420 · 23 May 2026 · ~7 min read
A presentation we regularly see in clinic is the frustrated patient who presents with back pain that was aggravated when attempting to strengthen their core. Whether that was Pilates, gym work, or a structured rehabilitation program — the activity they chose to strengthen and protect their back actually made it worse. They’d followed the standard advice and got the opposite of what they expected. The intricate anatomy of the low back — and more specifically, the thoracolumbar fascia — can help to explain why this may have occurred.
There is a structure in your lower back that most people have never heard of — and yet three separate anatomical studies, all published in the same journal, have argued it may be one of the most mechanically important junctions in the lumbar spine. It is called the lateral raphe. And understanding it changes the way you think about core training, back rehabilitation, and why treating either your paraspinal muscles or your abdominal muscles in isolation often misses the point.
What we knew — and what was missing
For decades, the thoracolumbar fascia (TLF) has been recognised as more than just wrapping around the lower back muscles. It is a broad, multi-layered sheet of connective tissue that serves as an attachment point for at least a dozen muscles — from the latissimus dorsi and gluteus maximus down to the transversus abdominis and internal oblique. Willard and colleagues (2012) produced what is now the definitive modern review of TLF anatomy, describing three distinct layers: the posterior layer (PLF), the middle layer (MLF), and the anterior layer — each with different mechanical properties, different muscle attachments, and different roles in load distribution. [1]
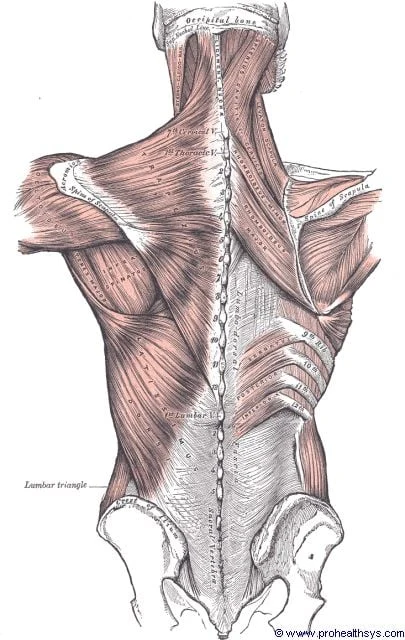
The thoracolumbar fascia — the broad white band spanning the lumbar region. At least a dozen muscles attach to its three layers, including the latissimus dorsi and gluteus maximus above and the transversus abdominis and internal oblique anterolaterally. The lateral margin of this structure — the lateral raphe, visible as the outer edge of the white band — is the load-distribution node that is the subject of this article. Illustration: Henry Vandyke Carter, Gray's Anatomy (1918) — public domain.
What the research had not yet fully resolved was how all of these muscles, pulling in different directions, actually coordinate their forces through the TLF — and where, structurally, that coordination happens.
The lateral raphe is part of the answer.
The term was first coined by Bogduk and MacIntosh in 1984 to describe a thickened ridge of connective tissue along the outer edge of the paraspinal muscles, roughly from the iliac crest up to the 12th rib. They described it as the point where the abdominal muscle aponeuroses joined the fascial structures of the back. But what exactly was happening at that junction, at the level of the tissue itself, remained poorly understood.
Three studies that built on each other
Study 1: Mapping what the lateral raphe actually is
In 2012, Schuenke and colleagues set out to characterise the anatomy of the lateral margin of the TLF in detail. Their dissections — on 12 embalmed cadavers plus 37 MRI sequences covering 898 individual lateral margins — confirmed something that had not previously been described: a fat-filled triangular space sitting at the core of the lateral raphe. [2]
They named it the lumbar interfascial triangle, or LIFT.
Here is what creates it. The paraspinal muscles are enclosed within their own continuous fascial sheath — the paraspinal retinacular sheath (PRS) — running from the spinous processes medially to the transverse processes laterally. As the aponeurosis of the transversus abdominis (TrA) and internal oblique (IO) approaches the outer edge of this sheath, it splits into two separate layers. One layer attaches to the front wall of the PRS; the other attaches to the back wall. The triangular space between those two laminae, and the portion of the PRS bridging them, is the LIFT.
The LIFT was identified in 84.3% of MRI sequences at the L1–L4 levels. It is not a rare anatomical variant — it is a consistent structural feature of the lumbar spine.
The lateral raphe, then, is not simply a line on a diagram. It is the ridged union of dense connective tissue that forms at the surface of the LIFT — the visible result of multiple fascial sheaths converging at this junction. It is where the abdominal myofascial girdle hands off its tension to the paraspinal fascial system, and vice versa.
Study 2: What force actually travels through it
Knowing the anatomy is one thing. Understanding the mechanics is another. Barker and colleagues (2004) had already demonstrated, using strain gauges on unembalmed cadavers, that tensioning the TrA/IO aponeurosis transmits measurable force to both the PLF and the MLF — and that the highest strain concentrations occur at the lateral raphe. [3]
The question that Vleeming and colleagues (2014) then asked was subtler: does it matter whether the paraspinal muscles are also active? Or does TrA tension alone do the job? [4]
Their method was ingenious. In seven unembalmed cadavers, they surgically removed the lumbar paraspinal muscles and replaced them with inflatable rubber tubes. Inflating the tubes simulated paraspinal muscle contraction by generating outward pressure on the PRS. They then measured what happened to the PLF and MLF under four conditions: baseline, TrA/IO tension alone (via the common tendon, or CTrA, at 8.5 N per side), paraspinal inflation alone, and both together.
The results were clear.
Paraspinal inflation alone significantly increased the perimeter of the PLF and caused it to displace posteriorly — creating what amounts to a greater extension moment arm for the paraspinal muscles, consistent with the hydraulic amplifier mechanism described by Gracovetsky and Bogduk. The MLF, however, did not change under any loading condition (P = 0.78).
When both paraspinal inflation and CTrA tensioning were applied together, force was preferentially and synergistically directed to the PLF (P = 0.0001). The maximum posterior expansion of the PLF in the combined condition was 1.56 cm.
In other words: the PLF is the primary load-bearing layer in this system. The MLF is not. And the system works best when both the paraspinal muscles and the abdominal girdle are active together.
The authors described this as a “co-dependent coupling mechanism” — and proposed that a “point of equal tension” exists between the two muscle groups, mediated through the lateral raphe junction.
Study 3: The broader picture
The Willard 2012 review [1] provides the anatomical context that ties these findings together. The TLF is not simply a passive wrapper. Its posterior layer has tensile strength of up to 1 kN. It is innervated by mechanoreceptors (Ruffini corpuscles, Pacinian corpuscles) and nociceptors. Its stiffness is modulated not only by muscle contraction but by myofibroblasts — cells that can maintain chronic tension in the fascial sheath through a mechanism involving TGF-β1 and sympathetic nervous system activity. Willard and colleagues describe how this myofibroblast activity may explain the “frozen lumbar” presentation in some people with chronic low back pain — a pattern of fascial stiffening comparable in histological appearance to frozen shoulder.
The lateral raphe sits within this broader system. It is the structural node through which the competing and complementary pulls of the gluteus maximus, latissimus dorsi, TrA, IO, and paraspinal muscles are integrated and distributed across the TLF.
Why this matters for the way we approach low back pain
These three studies converge on a simple but important clinical implication: the lumbar stabilisation system is not a collection of individual muscles you can address one at a time. It is a coupled system, and the lateral raphe is the coupling point.
Research has consistently shown that low back pain is associated with reduced cross-sectional area and delayed activation of the lumbar multifidus, and with altered timing of TrA contraction. [5] The Vleeming 2014 findings suggest why this matters mechanically: if paraspinal function is impaired, the outward pressure on the PLF is reduced, the extension moment arm shortens, and the CTrA alone cannot compensate. The girdling relationship between the abdominal and paraspinal systems — mediated through the LIFT and lateral raphe — is disrupted.
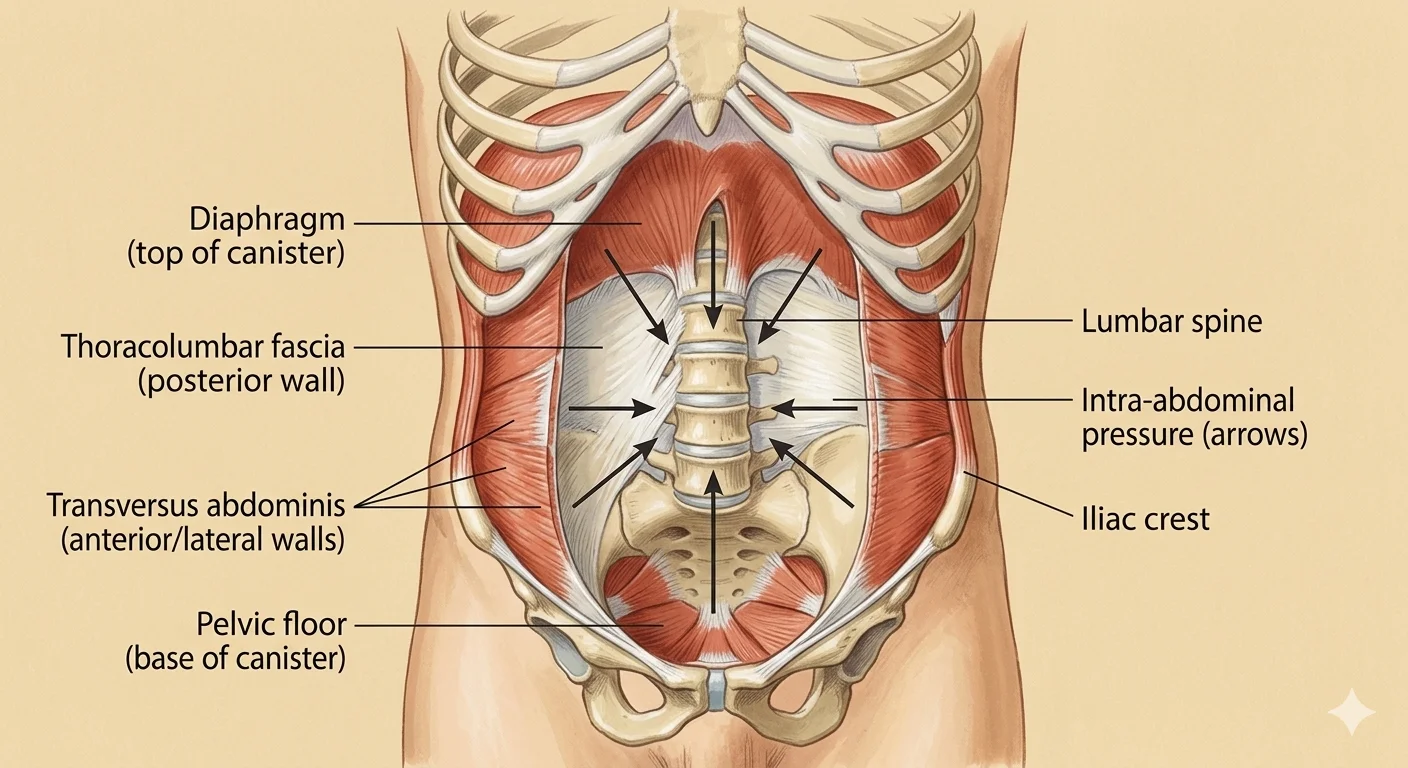
The abdominal canister: diaphragm above, pelvic floor below, transversus abdominis and multifidus forming the cylinder walls. Tension generated by TrA is transmitted to the thoracolumbar fascia at the posterior wall — but the Vleeming 2014 data show this mechanism works most effectively when paraspinal co-activation loads the PLF simultaneously. Neither component is sufficient alone; the lateral raphe is where their combined tension is distributed.
This is why, in clinical practice, we assess the whole system — not just where the pain is. A person presenting with lumbar pain may have perfectly adequate TrA function in an isolated test, but the moment that function is needed alongside loaded paraspinal activity — picking something up from the floor, decelerating from a run — the coupling fails.
We also view this through a fascial lens in a more specific sense — and this is where the Stecco Fascial Manipulation method has something specific to offer.
The LA-LU point: fascial manipulation at the lateral raphe
Within the Fascial Manipulation framework, the lateral raphe region corresponds to a treatment point known as LA-LU — the lateral lumbar centre of coordination. It sits in the quadratus lumborum area at the lateral border of the paraspinal muscles, precisely where the abdominal aponeuroses converge on the paraspinal retinacular sheath at the LIFT.
When this junction becomes densified — when the hyaluronan (HA) in the loose connective tissue at the LIFT loses its normal fluid state and thickens into a more viscous gel — the gliding between the abdominal and paraspinal fascial layers is impaired. [6] The result is not necessarily pain at the raphe itself. It can manifest as restricted lateral bending, altered rotation, altered load distribution under bending or carrying — or pain referred elsewhere along the lateral fascial sequence, anywhere from the ankle to the cervical spine.
This is one reason the Fascial Manipulation approach does not treat symptoms in isolation. LA-LU is rarely, if ever, assessed in isolation — and the rationale extends well beyond the lumbar region.
The lateral fascial sequence of which LA-LU is one point runs continuously from the lateral ankle and knee, through the lateral hip and iliotibial region, through the lateral lumbar territory, and into the lateral thoracic and cervical spine. Tension travels along this sequence in both directions. A densification or restriction at any point along it — a chronic lateral ankle restriction, a densified lateral hip, a stiff iliotibial region — alters the mechanical input arriving at the lateral raphe. The disruption may be well above or below the pain site. This is why the full sequence is assessed from top to bottom, not just the lumbar segment where symptoms are felt.
The picture is broader still. The lateral raphe is a convergence point — not just for the lateral sequence, but for multiple myofascial sequences. The posterior oblique sling, the anterior oblique sling, and even the anterior sequences (through their influence on abdominal muscle function) can all alter how load is shared through the LIFT. When dysfunction is present in any sequence whose tension passes through this junction, the co-dependent coupling mechanism that Vleeming and colleagues described can be compromised — regardless of which sequence is the primary driver.
The corollary is important: low back pain does not automatically point to LA-LU as the relevant treatment site. For many people, the dysfunction that is altering lateral raphe load-share sits in a different sequence entirely — and the clinical assessment determines that, not the location of the pain.
Importantly, the antagonistic side is always assessed as well. If a myofascial sequence on one side of the body is densified, the opposing sequence is typically under compensatory load. Addressing only the symptomatic side tends to produce incomplete or short-lived results.
The treatment itself is directed at restoring gliding at the LIFT junction. Your practitioner applies localised friction — perpendicular and oscillating rather than constant sliding — to the densified area. Research modelling HA flow during different manual therapy motions has shown that oscillatory and perpendicular techniques generate substantially greater fluid pressure in the HA layer than constant sliding, driving HA toward the fascial edges and increasing the interfascial gap. [7] This local pressure and heat is thought to be sufficient to shift HA from its gel state back toward a more fluid state, restoring the gliding capacity of the LIFT junction. [8] The aim is not to force a structural change — it is to restore the normal mechanical environment in which the LIFT can do its job: distributing tension from the abdominal girdle and the paraspinal muscles across both layers of the thoracolumbar fascia.
When this junction is moving freely, the co-dependent mechanism that Vleeming and colleagues described — the synergistic loading of the PLF under combined paraspinal and TrA activity — can operate as designed.
What this means for you
If you have been doing core exercises — planks, bird-dogs, drawing-in — and your back pain has not shifted, it is worth asking whether the training approach is actually loading the system in the way the research describes.
A few practical points:
- Isolated TrA training has its place, but it is not the whole story. The Vleeming 2014 data show that TrA tension alone produces substantially less PLF loading than TrA plus paraspinal activation together. Rehabilitation approaches that restore coordinated co-activation — rather than sequential, isolated muscle work — are more consistent with the mechanical evidence.
- The lumbar multifidus matters. The paraspinal component of this system is not optional. If the multifidus has atrophied following an acute injury — which the literature suggests happens rapidly and does not reverse spontaneously — the co-dependent mechanism cannot function as designed.
- Movement patterns matter as much as strength. The lateral raphe is loaded during functional movement — gait, rotation, loaded bending — not just static core bracing. Rehabilitation that includes loaded movement, not just isolated exercise, is more likely to restore the coupling this system requires.
- If the fascial junction is restricted, exercises alone may not restore gliding. The LIFT is designed to distribute tension across the TLF — but if the connective tissue at this junction has densified, the mechanical coupling is compromised regardless of muscle strength. This is where a specific assessment of the lateral fascial system, not just the muscles around it, is worth considering.
- Bilateral assessment matters. If you have unilateral lumbar pain or restricted lateral bending on one side, the restricted side is rarely the whole story. The opposite side often carries compensatory load, and addressing only the symptomatic side may explain why some treatment approaches produce short-term improvement followed by return of symptoms.
Want to know if this applies to your situation?
Call Now — speak with our team
Book Online — available 24/7
References
- PubMed Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. (2012). The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of Anatomy, 221(6), 507–536.
- PubMed Schuenke MD, Vleeming A, Van Hoof T, Willard FH. (2012). A description of the lumbar interfascial triangle and its relation with the lateral raphe: anatomical constituents of load transfer through the lateral margin of the thoracolumbar fascia. Journal of Anatomy, 221(6), 568–576.
- PubMed Barker PJ, Briggs CA, Bogeski G. (2004). Tensile transmission across the lumbar fasciae in unembalmed cadavers: effects of tension to various muscular attachments. Spine, 29(2), 129–138.
- PubMed Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. (2014). The functional coupling of the deep abdominal and paraspinal muscles: the effects of simulated paraspinal muscle contraction on force transfer to the middle and posterior layer of the thoracolumbar fascia. Journal of Anatomy, 225(6), 447–462.
- PubMed Hodges PW, Richardson CA. (1996). Inefficient muscular stabilization of the lumbar spine associated with low back pain. Spine, 21(22), 2640–2650.
- PubMed Stecco C, Stern R, Porzionato A et al. (2011). Hyaluronan within fascia in the etiology of myofascial pain. Surgical and Radiologic Anatomy, 33, 891–896.
- PubMed Roman M, Chaudhry H, Bukiet B, Stecco A, Findley TW. (2013). Mathematical analysis of the flow of hyaluronic acid around fascia during manual therapy motions. Journal of the American Osteopathic Association, 113(8), 600–610.
- PubMed Ercole B, Stecco A, Day JA, Stecco C. (2010). How much time is required to modify a fascial fibrosis? Journal of Bodywork & Movement Therapies, 14(4), 318–325.
Please note: This post is intended for educational purposes only and does not constitute clinical advice. Individual presentations vary. Please consult a registered health practitioner for advice about your specific condition.