Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Is Migraine?
Migraine is a complex neurological disorder characterised by recurrent episodes of moderate to severe headache — typically unilateral, pulsating in quality, lasting 4–72 hours, and accompanied by nausea, vomiting, and significant sensitivity to light and sound. Approximately one-third of people with migraine experience aura — transient neurological symptoms (most commonly visual) that precede or accompany the headache phase.
Migraine is significantly more prevalent than commonly appreciated — affecting approximately 12% of the general population and representing a leading cause of years lived with disability globally. It is disproportionately prevalent in women (3:1 ratio over men) and peaks in the most productive working decades.
The underlying neurobiology of migraine involves cortical spreading depression, trigeminovascular activation, and sensitisation of the trigeminal pain pathways. These processes are real, complex, and not fully within the scope of musculoskeletal care. Our focus here is on the cervical musculoskeletal component — the part of the clinical picture that manual therapy and rehabilitation can meaningfully influence.
| Feature | Detail |
|---|---|
| Character | Moderate to severe, unilateral, pulsating |
| Duration | 4–72 hours per episode (untreated or unsuccessfully treated) |
| Associated features | Nausea, vomiting, photophobia, phonophobia |
| Aura | Transient neurological symptoms in ~30% — visual most common |
| Prevalence | ~12% general population; 18% women; 6% men |
| Migraine + neck pain | Neck pain present in 75% of migraine attacks; often prodromal |
| Common triggers | Hormonal changes, sleep disruption, stress, skipped meals, alcohol, sensory stimuli |
| Cervical component | Upper cervical restriction and pericranial trigger points common in migraineurs |
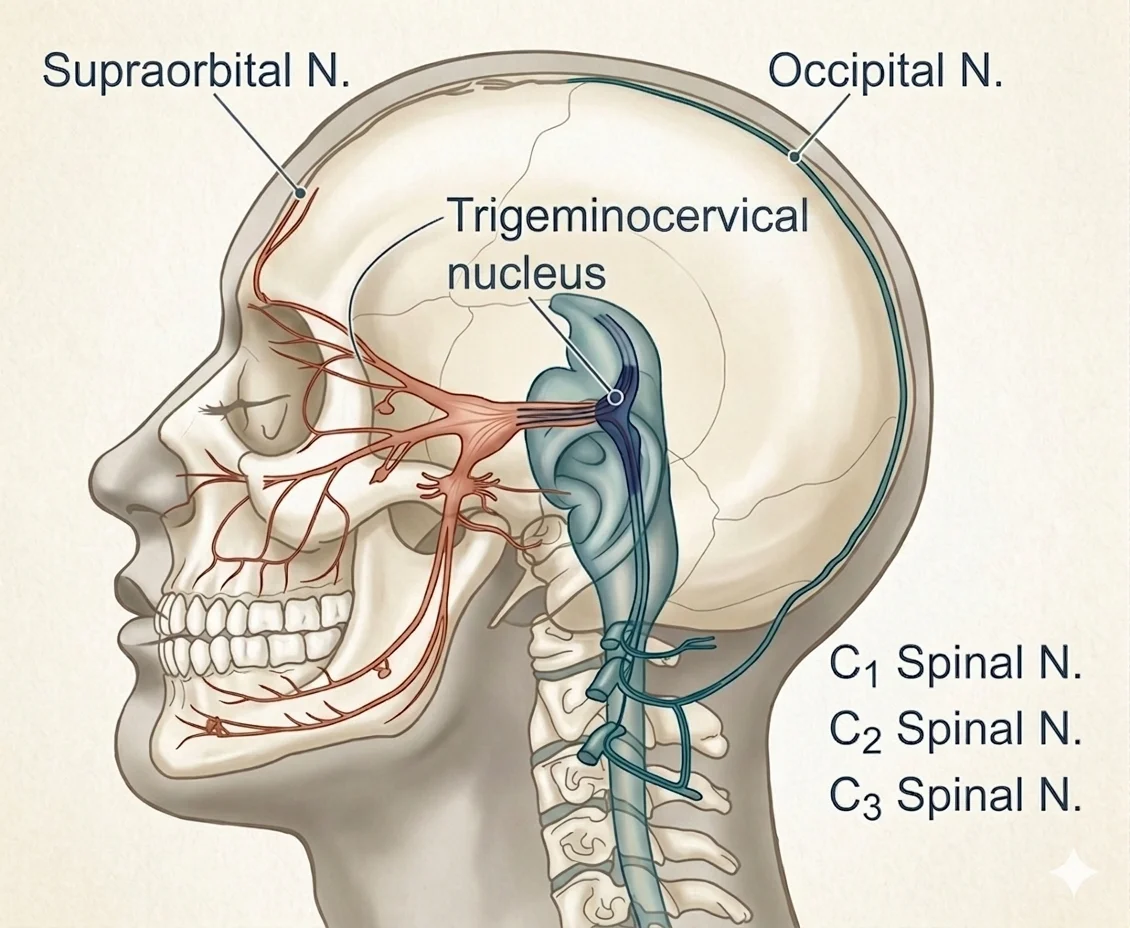
The trigeminocervical nucleus (TCN) — the brainstem region where trigeminal pain signals from the face and meninges converge with upper cervical sensory input (C1–C3). This convergence is central to the musculoskeletal contribution to migraine: cervical sensitisation at the TCN lowers the threshold for trigeminal activation, making attacks more likely and harder to abort once triggered. Upper cervical joint restriction and fascial densification directly sensitise this pathway — which is why manual therapy targeting C1–C3 can reduce migraine frequency even without touching the head.
Who Typically Experiences This?
People With Frequent Episodic or Chronic Migraine
When migraine occurs 8 or more days per month (episodic high-frequency) or 15 or more days per month (chronic migraine), the cumulative burden of attacks — including the post-drome recovery period — affects daily function substantially. This population typically has well-established cervical musculoskeletal impairments: forward head posture, restricted flexion-rotation test, reduced cervical flexor endurance, and active pericranial trigger points. Addressing these impairments is not a cure for migraine, but may reduce the frequency and severity of attacks.
Desk Workers With Poor Cervical Posture
Forward head posture maintains the cervical and suboccipital tissues in a state of sustained mechanical load, sensitising the pericranial and perivertebral structures that feed into the trigeminal pain system. The trigeminocervical nucleus — where cervical afferents (C1–C3) converge with trigeminal afferents — is the anatomical junction that explains why upper cervical dysfunction can lower the migraine threshold. A person who might have one migraine per month without cervical loading may have three or four per month with it. The posture isn't causing the migraine; it's lowering the threshold for each attack.
Women in the Perimenopausal Period
The intersection of hormonal fluctuation and cervical musculoskeletal loading is a particularly common clinical picture. Hormonal changes in the perimenopausal period significantly increase migraine frequency. If coexisting cervical impairments are raising the baseline trigeminocervical sensitivity, the hormonal trigger has less threshold to overcome — attacks become more frequent. Managing the cervical component does not resolve the hormonal driver, but may reduce overall attack frequency.
People Whose Migraine Began After Whiplash or Cervical Trauma
Post-traumatic migraine following whiplash injury is a well-recognised pattern. Cervical afferent sensitisation from upper cervical facet joint damage or capsular injury following rapid acceleration-deceleration creates a persistently lowered trigeminocervical threshold. People in this category frequently have identifiable upper cervical restriction and a positive Flexion-Rotation Test, and tend to respond particularly well to upper cervical manual therapy.
The Fascial Lens: Why the Cervical Spine Matters in Migraine
The trigeminocervical nucleus caudalis is the anatomical bridge between the migraine neurobiology and the cervical spine. It is a region of the spinal trigeminal nucleus that extends from the caudal brainstem down to approximately C3 — and it receives converging afferent input from both the trigeminal nerve (supplying the face, scalp, dura, and meningeal vessels) and the upper cervical spinal nerves (C1, C2, and C3, supplying the upper cervical joints, suboccipital muscles, and posterior scalp).
This convergence means that peripheral sensitisation from the upper cervical joints and suboccipital fascia can lower the excitability threshold of the trigeminocervical system — making it more susceptible to migraine activation from other triggers (hormonal, metabolic, sensory). The reverse is also true: migraine attacks themselves sensitise the trigeminocervical system, which is part of why neck pain is so frequently prodromal or ictal in migraine (present in approximately 75% of migraine attacks).
The practical clinical implication: upper cervical joint restriction, suboccipital fascial densification, and pericranial trigger points are not just accompanying findings in migraineurs — they are sources of ongoing afferent input into a sensitised trigeminocervical system. Reducing that input, by restoring upper cervical mobility and addressing the pericranial fascial and muscular environment, aims to raise the threshold for attack initiation.
The Flexion-Rotation Test (FRT) — a passive test of upper cervical rotation in full flexion — is particularly useful in this population. Restricted and painful FRT indicates upper cervical (C1–C2) restriction. In people whose migraine has a dominant cervical component, FRT restriction is commonly found and responds to targeted upper cervical mobilisation.
What Does the Research Say?
Spinal manipulation reduces migraine days and pain intensity. A systematic review and meta-analysis by Rist and colleagues (2019, Harvard Medical School) identified 6 RCTs (pooled n=677) evaluating spinal manipulation for migraine. After excluding one trial with high heterogeneity (chronic migraine only), the remaining 5 RCTs showed low heterogeneity. Spinal manipulation significantly reduced migraine days (Hedges' g = −0.35; 95% CI −0.53, −0.16; p<0.001) and migraine pain/intensity. The authors characterise the results as preliminary and note the need for larger methodologically rigorous trials — but the direction and consistency of effect across multiple RCTs is supportive. [1]
Cervical musculoskeletal impairments are measurably present in migraineurs. An updated systematic review and meta-analysis by Pensri and colleagues (2025, University of Queensland) included 77 studies (2551 participants) and found that people with migraine had significantly increased forward head posture in standing (MD −2.51°), reduced flexion/rotation range (MD −9.47°), and reduced cervical flexor and extensor strength and endurance compared to controls. Pericranial trigger points and tenderness were common, particularly in chronic migraine. [2]
A 2026 CPG recommends spinal manipulation for cervicogenic headache — a condition that overlaps significantly with migraine's cervical component. The Trager et al. CPG (2026), developed through Delphi consensus of 57 clinicians reviewing 32 systematic reviews, provides strong recommendations for spinal manipulation in cervicogenic headache. The upper cervical mechanism that drives cervicogenic headache — C1–C3 afferent sensitisation of the trigeminocervical system — is the same mechanism that contributes the cervical component to migraine. The evidence base for upper cervical manual therapy in cervicogenic headache is therefore mechanistically relevant to migraine with a dominant cervical contribution. [3]
Manual therapy in patients with migraine and concurrent cervical involvement — findings from a 2026 RCT. Amons and colleagues (2026, Archives of Physiotherapy) conducted an RCT of manual therapy versus usual GP care in 67 patients with migraine and neck pain (12-week intervention, 52-week follow-up). Manual therapy did not outperform usual care on the primary outcome of migraine day frequency. However, manual therapy produced significantly higher pressure pain thresholds over the occipital region at all follow-up points (p<0.01), greater patient-perceived recovery at 12 weeks (p=0.02) and 52 weeks (p<0.01), and significantly fewer other headache days at 52 weeks (p=0.03). Notably, use of prophylactic medication was substantially higher in the usual care group at all time points (p<0.001), which may partially explain comparable migraine day counts between groups. A co-investigator is from the same research group as Paper 186 (De Hertogh et al. 2025 cervicogenic dizziness). These findings suggest that manual therapy directed at the cervical component may produce measurable changes in local sensitisation and patient-reported recovery, even when the primary headache frequency outcome is not significantly altered. [4]
How We Approach Migraine — The Musculoskeletal Component
We are explicit about the scope and intent of what we do in migraine: we assess and treat the cervical musculoskeletal component. We do not treat migraine as a whole. For many people with migraine, neurological management — preventive medications, acute abortive therapy, trigger management — is an appropriate primary approach. Our work is complementary to that, not a replacement for it.
Our assessment includes the Flexion-Rotation Test, upper cervical segmental assessment (C0–C3), suboccipital muscle and fascial evaluation, pericranial trigger point assessment, and cervical strength and endurance screening. We identify the degree to which cervical musculoskeletal impairment is present and contributing to the clinical picture.
Where upper cervical restriction is identified, mobilisation directed at C1–C2 and C2–C3 is the primary manual therapy intervention. Fascial Manipulation addresses the posterior cervical and suboccipital centres of coordination where densification within the fascial system is maintaining suboccipital tension. Trigger point therapy addresses pericranial sensitisation at the temporalis, suboccipital, and upper trapezius.
Exercise prescription focuses on deep cervical flexor strengthening, postural retraining, and thoracic mobility — addressing the cervical impairments identified in the research as consistently present in migraineurs.
We work collaboratively with the person's treating GP and neurologist where appropriate. Reducing the cervical musculoskeletal contribution to migraine frequency and threshold is a meaningful clinical goal, even where the migraine neurobiology remains a primary management focus.
New to Fascial Manipulation? Read how it works → · How chiropractic adjustments work →
Please note: The information on this page describes our general clinical approach to the musculoskeletal component of migraine and is intended for educational purposes only. Migraine is a complex neurological condition and requires appropriate medical evaluation and management. Nothing on this page constitutes advice to change or discontinue medical treatment for migraine. New, severe, sudden-onset, or progressively worsening headache requires urgent medical evaluation. Individual presentations vary, and your assessment and management will be tailored specifically to you. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Track whether your neck symptoms precede your migraine attacks.
Neck stiffness, suboccipital tightness, or upper cervical aching in the hours before a migraine (the prodrome) suggests a cervical musculoskeletal contribution that may be modifiable. Keeping a brief headache diary — noting neck symptoms, time of day, sleep quality, and any identifiable triggers — for 4–6 weeks gives a clearer picture of this relationship.
2. Assess your cervical mobility.
A simple screen: sit upright, nod your chin to your chest to maximally flex the cervical spine, then try to rotate your head left and right in that position. This is a rough self-assessment of the Flexion-Rotation Test. Normal rotation is approximately 45° each side in full flexion. If one side is significantly more restricted or painful, this is worth investigating — upper cervical restriction at C1–C2 is a common and treatable finding in migraineurs.
3. Address forward head posture as a baseline intervention.
The cervical musculoskeletal impairments documented in research (forward head posture, reduced flexor endurance) are all worsened by sustained forward head position. Screen height at eye level, regular chin tuck exercises (cervical retraction), and upper thoracic extension work over a foam roller are the most impactful basic interventions. These don't cure migraine, but they reduce the chronic cervical afferent load on the trigeminocervical system.
4. Communicate your cervical findings to your neurologist or GP.
If you have identified upper cervical restriction or pericranial trigger points through assessment, this information is relevant to your overall migraine management. A collaborative approach — musculoskeletal care for the cervical component alongside appropriate medical management — is more likely to reduce overall attack frequency than either approach in isolation.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
The musculoskeletal contribution to migraine operates through the trigeminocervical nucleus — where cervical spine input lowers the threshold for central sensitisation and migraine triggering. This pillar article maps the full cervical and fascial context relevant to migraine management.
Read Article →Migraine involves the same brainstem convergence pathways as cervicogenic headache and dizziness — the trigeminal, cervical, and vestibular systems all feed into a shared nucleus whose sensitivity determines migraine threshold. This article explains the neuroanatomy linking the neck, jaw, and headache.
Read Article →References
- PubMed Rist PM, Hernandez A, Bernstein C, Kowalski M, Osypiuk K, Vining R, Long CR, Goertz C, Song R, Wayne PM (2019). The Impact of Spinal Manipulation on Migraine Pain and Disability: A Systematic Review and Meta-Analysis. Headache, 59(4), 532–542.
- PubMed Pensri C, Liang Z, Treleaven J, Jull G, Thomas L (2025). Cervical musculoskeletal impairments in migraine and tension-type headache and relationship to pain related factors: An updated systematic review and meta-analysis. Musculoskeletal Science and Practice, 76, 103251.
- PubMed Trager RJ, Daniels CJ, Hawk C, et al. (2026). Chiropractic Management of Adults with Cervicogenic or Tension-Type Headaches: Development of a Clinical Practice Guideline. Journal of Integrative and Complementary Medicine. DOI: 10.1177/27683605251397769.
- PubMed Amons AL, Castien RF, De Hertogh W, Knoop H, van der Windt DAWM, Leeuw M (2026). Effectiveness of manual therapy as a prophylactic treatment for migraine: a randomised controlled trial. Archives of Physiotherapy, 16, 11–22.