Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Are Temporomandibular Disorders?
Temporomandibular disorders (TMD) is an umbrella term for a group of musculoskeletal conditions involving the temporomandibular joint (TMJ), the masticatory muscles, and associated orofacial structures. TMD affects approximately 6–9% of adults globally and is twice as prevalent in women as in men. It is the leading cause of chronic non-odontogenic orofacial pain.
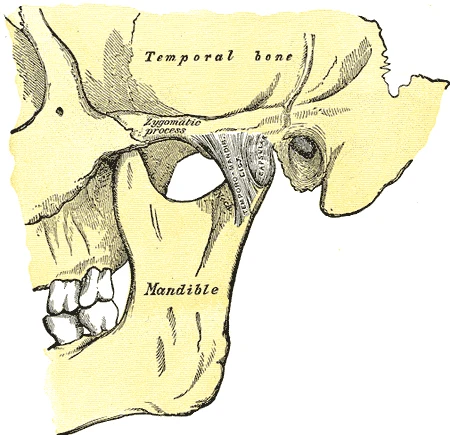
The TMJ is one of the most mechanically complex joints in the body. It combines hinge and glide movement within a single joint space, separated by an articular disc, and is mobilised by the most powerful muscles per unit area in the human body — the masseter, temporalis, and medial pterygoid. Both the joint itself and the masticatory muscles are richly innervated by branches of the trigeminal nerve (cranial nerve V), which also supplies the face, scalp, and dura — which explains why TMD frequently presents with headache, facial pain, and ear symptoms alongside the jaw itself.
| Feature | Detail |
|---|---|
| Structures involved | TMJ (condyle, disc, capsule), masticatory muscles (masseter, temporalis, pterygoids), ligaments |
| Prevalence | 6–9% adults globally; second most common MSK chronic pain condition |
| Common symptoms | Jaw pain, limited or asymmetric mouth opening, clicking or crepitus, temporal headache, ear pain, neck pain |
| Key provocations | Jaw opening, chewing, jaw clenching, yawning, sustained dental work |
| Diagnosis | Research Diagnostic Criteria for TMD (RDC/TMD); no single definitive test |
| Comorbidities | Cervical spine dysfunction, headache, bruxism, sleep disturbance, stress |
| Who is affected | Women > men; typically 20–40 years; but any age |
TMD is broadly classified into three categories that frequently overlap:
- Myofascial pain — pain originating in the masticatory muscles and their fascial investments
- Internal derangements — disc displacement with or without reduction
- Degenerative joint disease — osteoarthritis of the condyle-disc-eminence complex
Who Typically Experiences This?
People With Bruxism or Jaw Clenching
Nocturnal bruxism (tooth grinding during sleep) and diurnal jaw clenching (habitual daytime clenching, often stress-associated) are among the most common drivers of masticatory muscle overload. The masseter and temporalis are the primary muscles involved, and their sustained or repetitive contraction beyond normal physiological load drives myofascial sensitisation, trigger point formation, and progressive joint loading. Many people are unaware they clench — it often surfaces through dental wear, jaw fatigue on waking, and morning temporal headaches.
Desk Workers and Sustained Jaw Loading
Forward head posture — the habitual working posture of most desk workers — alters the resting position and mechanics of the mandible. In a forward head position, the mandible tends to rest with the teeth slightly apart and the condyle in a slightly inferior-anterior position, which can alter the joint load distribution and masticatory muscle activation patterns. This is one mechanism through which desk work posture contributes to TMD without any direct jaw trauma.
People Under Significant Psychological Stress
The relationship between psychological stress and TMD is well-established. Stress activates the sympathetic nervous system and increases masticatory muscle tone, peripheral pain sensitisation, and central pain amplification. People under significant occupational, relational, or financial stress are disproportionately represented in TMD presentations — and management that addresses only the joint without the stress-associated masticatory muscle hyperactivation is often insufficient.
People With Cervical Spine Dysfunction
This is the most clinically important association for our practice: cervical spine dysfunction and TMD co-occur at a rate far above chance. The anatomical basis is the trigeminocervical nucleus — the same brainstem region where cervical afferents (C1–C3) converge with trigeminal afferents (supplying the jaw, face, and dura). Sensitisation from the upper cervical spine lowers the threshold for trigeminal pain, and vice versa. A 2020 systematic review and meta-analysis confirmed a clinically significant association between neck disability and jaw disability (SMD 0.72), and documented reduced cervical ROM and lower pressure pain thresholds in people with TMD. Assessing and treating the cervical spine in TMD is not an optional add-on — it is a core component of comprehensive management. [1]
The Fascial Lens: Why We See This Differently
The masticatory system is embedded in and connected to the craniocervical fascial complex. The masseter, temporalis, and pterygoid muscles are invested by the masseteric fascia, temporal fascia, and pterygoid fascia respectively — continuous extensions of the deep cervical fascial system that invests the muscles of the neck and anterior chest. The cervical fascia ascends through the parotid region and blends with the masseteric fascial layer; tension in the cervical fascial system is therefore transmitted into the jaw region, and vice versa.
The superficial layer of the deep cervical fascia — the investing layer — wraps the sternocleidomastoid, trapezius, and masseteric structures as a continuous sleeve. When this system is under chronic tension from sustained forward head posture, psychological stress, or jaw clenching, the masticatory muscles operate within a mechanically compromised fascial environment. The trigger points that develop in the masseter and temporalis are not isolated findings; they are expressions of a fascially connected system under load.
The myofascial component of TMD — masticatory muscle pain — is the subtype most responsive to manual therapy and fascial work. This is consistent with the mechanism: myofascial trigger points in the masseter, temporalis, and pterygoid muscles are maintained by the same densification process described in other fascial compartments throughout the body. Addressing the fascial tension in the craniocervical system — including the posterior cervical retinacular sheath, the suboccipital compartment, and the anterior cervical fascia — is a meaningful part of managing the myofascial component of TMD alongside direct treatment of the jaw.
What Does the Research Say?
A landmark BMJ clinical practice guideline strongly recommends manual mobilisation, trigger point therapy, and supervised exercise for chronic TMD. The 2023 BMJ guideline by Busse and colleagues — developed using GRADE methodology and network meta-analysis, with an international panel including patients, clinicians, and methodologists — found that manual mobilisation with trigger point therapy, supervised postural and jaw exercises, and cognitive behavioural therapy (with or without biofeedback) are the most strongly supported interventions for chronic TMD pain. Manipulation and acupuncture receive conditional recommendations. Occlusal splints, arthrocentesis, botulinum toxin, gabapentin, and TENS are conditionally or strongly recommended against. Irreversible interventions (oral splints, discectomy) are strongly recommended against. [2]
Fascial Manipulation is at least as effective as botulinum toxin injections for myofascial jaw pain. A 2012 RCT by Guarda-Nardini and colleagues (University of Padova, with Antonio and Carla Stecco as co-authors) compared FM with botulinum toxin injections in 30 patients with RDC/TMD-diagnosed myofascial pain of the jaw muscles. Both treatments produced statistically significant pain improvement over time. FM was slightly superior for pain reduction; botulinum toxin was slightly superior for jaw range of motion at end of treatment. At 3-month follow-up, no clinically relevant differences between groups were found. FM — a conservative, reversible approach — produced outcomes comparable to an injection that temporarily paralyses the masticatory musculature. [3]
Fascial Manipulation produces faster functional recovery in TMD than conventional treatment. A 2022 RCT by Sekito and colleagues (Bioengineering) compared FM with conventional TMD treatment (occlusion-based). Both groups achieved significant pain reduction (VRS p<0.0001) and improved pain-free mouth opening (p<0.001). The FM group demonstrated significantly faster recovery of maximum unassisted mouth opening (T0 vs T1, p=0.001). The authors concluded FM is an effective, rapid, safe, and cost-effective approach prior to occlusion stabilisation, with Antonio Stecco (New York University) as a co-author. [4]
Cervical musculoskeletal impairment is a clinically significant finding in TMD. A systematic review and meta-analysis by Cuenca-Martínez and colleagues (2020, Journal of Clinical Medicine) examined 25 observational studies and found a statistically significant association between neck disability and jaw disability (SMD 0.72; 95% CI 0.56–0.82). Moderate evidence supported reduced cervical range of motion and lower pressure pain thresholds in people with TMD compared to controls. This confirms that cervical assessment is clinically necessary in TMD presentations, not supplementary. [1]
How We Approach Temporomandibular Disorders
Our assessment of TMD begins with the jaw and extends systematically into the craniocervical region. We assess the TMJ for disc mechanics, condylar position, and joint mobility. We assess the masticatory muscles — masseter, temporalis, and medial and lateral pterygoids — for myofascial trigger points, tenderness, and resting tone.
We assess the upper cervical spine (C0–C3) and the craniocervical fascial system — because the research and the anatomy both indicate that these structures are functionally and mechanically connected to the jaw. The Flexion-Rotation Test and upper cervical palpation identify the cervical component that is so commonly present alongside TMD.
Fascial Manipulation is directed at the masseteric, temporal, and pterygoid fascial layers, and at the craniocervical centres of coordination within the posterior cervical and suboccipital fascial system. Trigger point therapy addresses the masticatory muscle sensitisation directly. Manual joint mobilisation of the TMJ addresses disc mechanics and condylar mobility.
Postural rehabilitation — addressing forward head posture, deep cervical flexor conditioning, and jaw rest position — is integrated throughout, consistent with the BMJ guideline's emphasis on supervised postural and jaw exercises as a strongly recommended intervention.
We work alongside treating dentists and oral medicine specialists where occlusal management, splint therapy, or joint imaging is part of the patient's overall care.
New to Fascial Manipulation? Read how it works → · How chiropractic adjustments work →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. TMD presentations vary significantly, and some require dental, oral medicine, or specialist assessment — particularly where joint pathology, disc derangement, or occlusal factors are prominent. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Check your resting jaw position.
The teeth should rest slightly apart during the day — lips closed, teeth not touching. Unconscious tooth contact during concentration, stress, or screen work is one of the most common drivers of masticatory muscle overload. Place a small sticker on your screen as a reminder to check and release jaw tension throughout the day. This single habit change reduces cumulative jaw loading significantly.
2. Apply heat to the masseter and temporalis.
A warm pack applied to the jaw muscles for 10–15 minutes reduces masticatory muscle tone and local myofascial sensitivity. This can be done before meals if chewing is painful, or at the end of the day when jaw clenching has accumulated. Heat reduces the viscosity of the fascial ground substance and temporarily restores sliding between fascial layers — the same mechanism that manual therapy uses.
3. Modify provocative activities temporarily.
Hard, chewy, or large foods (bagels, raw carrots, thick sandwiches requiring wide opening) load the TMJ and masticatory muscles at end range. During an acute or symptomatic phase, a temporary reduction in jaw loading — softer foods, smaller bites, avoiding wide yawning — reduces the repetitive provocation that prevents recovery.
4. Address your neck and shoulder posture.
Forward head posture maintains the masticatory system in a mechanically disadvantaged position. The neck and jaw are fascially and neurologically connected. Regular chin tucks, thoracic extension over a foam roller, and attention to screen height all reduce the cervical load that perpetuates jaw sensitisation.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
TMD and cervical spine dysfunction are anatomically linked through the trigeminocervical nucleus — jaw pain, neck pain, headache, and dizziness share convergent brainstem pathways that explain their frequent co-occurrence. This article maps the full neck-jaw-brainstem connection.
Read Article →The fascial system connecting the mandible, hyoid, cervical spine, and thoracic inlet means that jaw dysfunction rarely exists in isolation from cervical mechanics. This pillar article explains the cervical fascial context that shapes both TMD and the headache and dizziness that accompany it.
Read Article →References
- PubMed Cuenca-Martínez F, Herranz-Gómez A, Madroñero-Miguel B, Reina-Varona Á, La Touche R, Angulo-Díaz-Parreño S, Pardo-Montero J, del Corral T, López-de-Uralde-Villanueva I (2020). Craniocervical and Cervical Spine Features of Patients with Temporomandibular Disorders: A Systematic Review and Meta-Analysis of Observational Studies. Journal of Clinical Medicine, 9(9), 2806.
- PubMed Busse JW, Casassus R, Carrasco-Labra A, Durham J, Mock D, Zakrzewska JM, et al. (2023). Management of chronic pain associated with temporomandibular disorders: a clinical practice guideline. BMJ, 383, e076227.
- PubMed Guarda-Nardini L, Stecco A, Stecco C, Masiero S, Manfredini D (2012). Myofascial Pain of the Jaw Muscles: Comparison of Short-Term Effectiveness of Botulinum Toxin Injections and Fascial Manipulation Technique. CRANIO, 30(2), 95–102.
- PubMed Sekito F, Pintucci M, Pirri C, Ribeiro de Moraes Rego M, Cardoso M, Soares Paixão K, Ribeiro da Silva V, Stecco A (2022). Facial Pain: RCT between Conventional Treatment and Fascial Manipulation® for Temporomandibular Disorders. Bioengineering, 9(7), 279.