Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Is Tietze's Syndrome & Costochondritis?
These two conditions are often used interchangeably but they are clinically distinct:
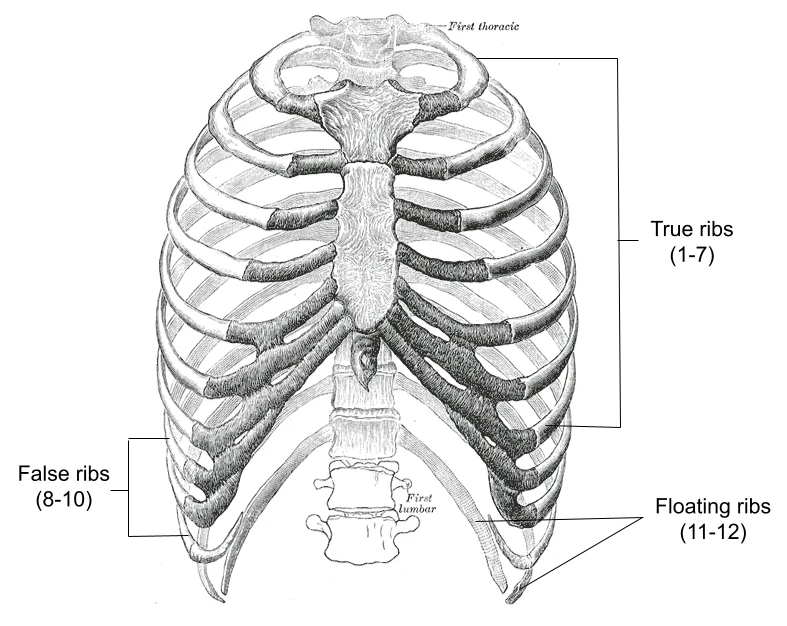
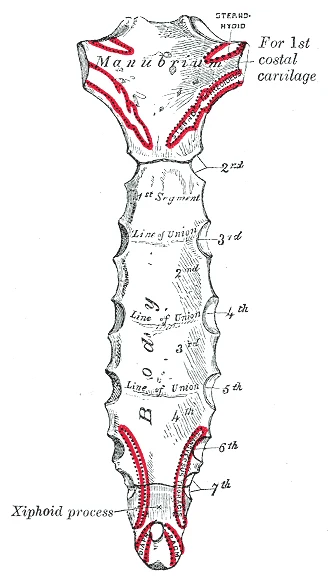
Tietze's syndrome is characterised by painful swelling at one or more costochondral junctions — the points where the costal cartilages meet the ribs. The swelling is visible and palpable, and is the defining feature that distinguishes Tietze's from costochondritis. It typically affects the upper costochondral junctions (second and third most commonly), is usually unilateral, and may be associated with trauma, upper respiratory infection, or repetitive mechanical loading.
Costochondritis presents with the same location of pain — anterior chest wall tenderness at one or more costochondral or costosternal junctions — but without swelling. It is far more common than Tietze's syndrome and is frequently described as a diagnosis of exclusion once cardiac, pulmonary, and gastrointestinal causes of chest pain have been ruled out.
Both conditions share the fundamental clinical feature: anterior chest wall pain that is reproduced by direct pressure on the costochondral junction and can be worsened by movements that load the rib cage — deep breathing, arm movement, coughing, sneezing, and twisting.
| Feature | Tietze's Syndrome | Costochondritis |
|---|---|---|
| Swelling | Present (visible/palpable) | Absent |
| Joints affected | Usually 2nd–3rd costochondral | Any costochondral/costosternal junction |
| Laterality | Usually unilateral | Can be bilateral |
| Typical onset | Trauma, infection, overuse | Insidious, often no clear precipitant |
| Prevalence | Rare | Common — up to 30% of acute chest pain presentations in primary care |
Who Typically Experiences This?
People Who Have Had Their Heart Cleared — And Are Still in Pain
The most common presentation we see is a patient who has been to the emergency department or seen their GP with chest pain, had cardiac causes excluded (ECG, troponin, chest X-ray), been diagnosed with "musculoskeletal chest pain" or costochondritis, and told to take anti-inflammatories and wait. When the pain continues for weeks or months, they present to us. The diagnosis is usually correct — but the treatment has been directed at the front when the mechanical driver is at the back.
Desk Workers
Sustained thoracic kyphosis — the postural profile of most desk-based workers — loads the anterior chest wall structures through a subtle but persistent compressive mechanism. The costochondral junctions bear the load of the rib cage resting in a flexed position. Over time, this cumulative anterior chest wall loading can sensitise the costochondral junctions, particularly at the levels of greatest thoracic kyphosis (T4–T7).
People Recovering From Respiratory Illness
Prolonged, forceful coughing — from COVID-19, influenza, bronchitis, or persistent post-viral cough — generates high repetitive forces at the costochondral junctions. The cough mechanism involves a rapid, forceful contraction of the thoracic cage muscles against a closed glottis, and the costovertebral and costochondral structures absorb this force. Post-viral costochondritis is a genuinely common presentation following significant respiratory illness.
Gym Athletes and Those With High Pressing Volumes
Heavy bench pressing, dumbbell chest work, and barbell rowing all load the anterior chest wall and the costovertebral articulations at the posterior thoracic spine simultaneously. Spikes in pressing volume are a common precipitant. Powerlifters and those doing high-volume upper body training are over-represented in costochondritis presentations relative to the general population.
The Fascial Lens: Why We See This Differently
The key insight — supported by both case report evidence and anatomical reasoning — is that costochondritis and Tietze's syndrome are often driven from the posterior thoracic spine, not the anterior chest wall.
Here is the anatomy that explains this:
The intercostal nerves (T2–T6) travel within the intercostal fascial compartments — the fascial spaces between the internal and innermost intercostal muscles — from the posterior costovertebral joints around the rib cage to the anterior chest wall. Their anterior terminal branches supply the costochondral junctions. This means that irritation or sensitisation of the intercostal nerve anywhere along its path — including at the posterior costovertebral and costotransverse joints — can produce pain and tenderness at the anterior costochondral junction where the nerve terminates.
When the posterior thoracic fascial environment is restricted — through the same postural loading and paraspinal densification that produces mid-back stiffness — the mechanical tension on the intercostal nerve increases. The result can be neurogenic sensitisation that presents anteriorly as costochondritis, while the posterior joint structures remain asymptomatic or mildly tender. This is the neurogenic inflammation model proposed by Rabey (2008) and supported by Stecco's research into fascial entrapment neuropathy.
This is why directing treatment at the anterior chest wall — topical NSAIDs, local injection, heat packs — often provides partial or temporary relief. The driver is posterior. Local treatment at the symptom site addresses the terminus of the problem, not its source. [1, 2]
It also explains why rib manipulation and posterior thoracic soft tissue work produces lasting resolution in cases where anterior treatment has failed — the intervention addresses the posterior mechanical and fascial environment that is producing the anterior symptoms. [3]
The anterior thoracic fascia is also relevant. The pectoral fascia, the clavipectoral fascia, and the perichondrium of the costal cartilages form a continuous anterior chest wall fascial layer. This layer bears load from the pectoral muscles during pressing movements and from the rib cage during sustained kyphosis. Densification within this layer can directly contribute to costochondral junction sensitisation independent of the posterior mechanism.
What Does the Research Say?
Manual therapy directed at the posterior thoracic spine and ribcage produces meaningful improvement in costochondritis. A retrospective case series by Zaruba and Wilson (2017) treated eight patients with costochondritis (mean duration 6.3 months) using an impairment-based approach targeting the cervicothoracic spine and ribcage with manual therapy and exercise. Subjects were seen an average of 4.8 times. The mean pain score reduced by 5.1 points (NPRS); mean functional score improved by 5.3 points (PSFS); mean global rating of change was 5.9. All subjects returned to their previous activities without restriction at discharge. The treatment was directed posteriorly — not at the anterior chest wall. [3]
Costochondritis may be driven by neurogenic inflammation from posterior segmental dysfunction. A case report by Rabey (2008) described two patients with clinical costochondritis who failed to respond to anterior chest wall treatment but achieved complete resolution following manual therapy directed at the posterior thoracic spine and rib articulations. The paper proposed that intercostal neurogenic inflammation — sensitisation of the intercostal nerve within its fascial compartment — produces the anterior chest wall signs, and that addressing the posterior segmental driver resolves the anterior presentation. [1]
Rib manipulation and soft tissue mobilisation can resolve persistent costochondritis. A 2021 case report (Barranco-Trabi et al.) documented complete resolution of a two-year history of atypical costochondritis — after extensive cardiac and gastroenterological evaluation — following three sessions of rib manipulation and instrument-assisted soft tissue mobilisation. The approach was framed around regional interdependence: testing whether posterior rib dysfunction was driving the anterior chest wall symptoms. Complete resolution was confirmed on examination. [2]
How We Approach Tietze's Syndrome & Costochondritis
Our assessment starts posteriorly — not anteriorly. We palpate and assess the costovertebral and costotransverse joints at the levels corresponding to the anterior chest pain, the surrounding paraspinal fascial tension, and the thoracic segmental mobility. We also assess the anterior chest wall directly, the pectoral fascial system, and the rib cage mechanics during breathing.
Where we identify posterior thoracic fascial restriction and costovertebral joint irritation at levels corresponding to the anterior symptoms, Fascial Manipulation is directed at the relevant centres of coordination within the paraspinal and intercostal fascial layers. Rib mobilisation addresses the specific posterior joint restrictions. Movement retraining addresses the breathing pattern, thoracic posture, and loading strategies that continue to drive anterior chest wall load.
We also assess pressing movement patterns in athletes — bench press setup, rib cage position, breathing under load — as these frequently reveal the mechanical context in which the anterior chest wall symptoms developed.
New to Fascial Manipulation? Read how it works → · How chiropractic adjustments work →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Anterior chest pain must be medically assessed to exclude cardiac, pulmonary, and other serious causes before a musculoskeletal diagnosis is attributed. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. First: exclude serious causes.
If you have not yet had anterior chest pain medically assessed — particularly if it is new, severe, associated with exertion, or accompanied by shortness of breath, palpitations, or arm/jaw pain — seek medical review before any musculoskeletal treatment. This is non-negotiable.
2. Reassess your thoracic posture and breathing mechanics.
Sustained thoracic kyphosis and shallow breathing patterns both increase anterior chest wall loading. Regular thoracic extension over a foam roller and deliberate diaphragmatic breathing throughout the day are low-risk self-management strategies that address the posterior mechanical environment.
3. Modify pressing volumes and technique.
If you are a gym athlete with costochondritis, a temporary reduction in pressing volume — bench press, dips, push-ups — reduces the repetitive anterior chest wall load while the tissues settle. Rib cage position during pressing (avoiding excessive flare) also reduces the shear force at the costochondral junctions.
4. Avoid sustained anterior thoracic loading.
Activities that involve sustained forward trunk flexion — extended desk work, driving, cycling — compress the anterior chest wall and costochondral junctions continuously. Regular extension breaks are particularly important during symptomatic phases.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
Breathing mechanics are directly implicated in costal cartilage and rib joint stress — when the diaphragm is underused and accessory muscles drive respiration, the upper ribs and sternocostal joints are subjected to repetitive abnormal load. This article explains the breathing-thoracic connection in detail.
Read Article →The thoracic cage, shoulder girdle and cervical spine share a continuous fascial envelope — altered thoracic mechanics from Tietze’s or costochondritis frequently produce secondary shoulder and neck tension. This pillar article maps the fascial connections relevant to anterior chest and shoulder presentations.
Read Article →References
- PubMed Rabey MI (2008). Costochondritis: are the symptoms and signs due to neurogenic inflammation? Two cases that responded to manual therapy directed towards posterior spinal structures. Manual Therapy, 13(1), 82–86.
- PubMed Barranco-Trabi J, Mank VM, Roberts J, Newman DP (2021). Atypical Costochondritis: Complete Resolution of Symptoms After Rib Manipulation and Soft Tissue Mobilization. Cureus, 13(4), e14369.
- PubMed Zaruba RA, Wilson E (2017). Impairment based examination and treatment of costochondritis: a case series. International Journal of Sports Physical Therapy, 12(3), 458–467.