Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Is Carpal Tunnel Syndrome?
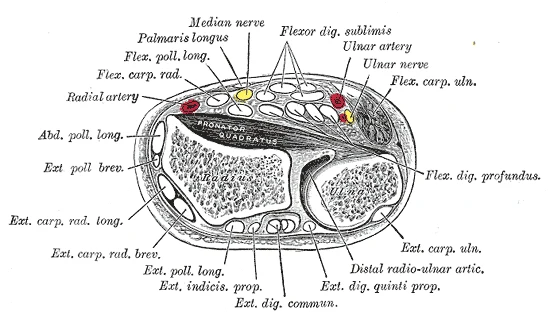
The carpal tunnel is a narrow passageway on the palm side of the wrist, formed by the carpal bones on three sides and the transverse carpal ligament — a thick fascial band — across the top. Through this tunnel pass nine flexor tendons and the median nerve. When pressure inside the tunnel rises, the median nerve is compressed, producing the characteristic symptoms of carpal tunnel syndrome (CTS).
The median nerve supplies sensation to the thumb, index, middle, and half of the ring finger, and controls the thenar muscles at the base of the thumb. Compression produces tingling and numbness in this distribution, often worse at night or with sustained wrist flexion (holding a phone, gripping a steering wheel). In more advanced presentations, there is weakness in fine pinch, difficulty with buttons or keys, and wasting of the thenar muscle bulk.
| Feature | Detail |
|---|---|
| Structure affected | Median nerve within the carpal tunnel |
| Key fascial structure | Transverse carpal ligament (flexor retinaculum) |
| Symptom distribution | Thumb, index, middle, radial half of ring finger |
| Classic provocation | Sustained wrist flexion, repetitive gripping, night symptoms |
| Population | Affects approximately 3–5% of the general adult population; peak incidence ages 40–60; more common in women |
| Diagnosis | Clinical (Phalen, Tinel, carpal compression test, Katz hand diagram) + nerve conduction studies where indicated |
Who Typically Experiences This?
Desk Workers and Remote Professionals
Sustained keyboard and mouse use maintains the wrist in a position that narrows the carpal tunnel and loads the flexor tendons. Over hours, this creates a low-grade, repetitive compression environment. Wrist rests that hold the wrist in flexion can make this worse. Many desk workers present with night symptoms first — the wrist falls into flexion during sleep, and the nerve's already sensitised state becomes symptomatic. Prolonged neck and shoulder postures in this population also contribute; the tissue environment along the entire upper limb is relevant.
Manual Workers and Tradies
Sustained grip, vibrating tools, and repetitive wrist flexion-extension are well-documented occupational risk factors for CTS. Construction workers, cleaners, and those in food preparation or manufacturing frequently present with bilateral symptoms. The combination of mechanical loading at the wrist and postural loading at the neck and shoulder is common in this population.
Gym Athletes and Weightlifters
Barbell work involving sustained wrist extension under load — particularly front rack position in Olympic lifting, overhead lifts, and high-volume pressing — can load the flexor compartment and the median nerve's course through the forearm. Grip-intensive training (deadlifts, pull-ups, farmer's carries) also repeatedly loads the flexor retinaculum. Athletes in this population often present with symptoms that are more activity-related than nocturnal.
Pregnant and Postpartum Women
CTS is common in pregnancy due to fluid retention increasing tunnel pressure, and in the postpartum period due to repeated lifting and carrying — particularly the wrist position involved in supporting an infant's head. This population frequently responds well to conservative management and often resolves with appropriate load modification, though symptoms can persist and require treatment.
Older Adults
Age-related changes in tendon volume, synovial thickening, and reduced tissue mobility can gradually narrow the tunnel. Older adults may present with a longer symptom history and a greater degree of sensory loss. This does not preclude conservative management, though the response timeline may differ.
The Fascial Lens: Why We See This Differently
The standard model of CTS frames it as a compression problem at the wrist: the tunnel is too small for its contents, the nerve gets squeezed, symptoms result. While this is anatomically accurate at the site, it doesn't fully explain why many people have the same anatomical tunnel dimensions and loading patterns — yet only some develop symptoms.
The concept that changes the picture is the neural container: the entire fascial environment through which the median nerve travels, from the cervical spine to the palm. At every step along that path, the nerve passes through or adjacent to fascial structures that can influence its mobility, its blood supply, and its sensitivity.
Starting proximally:
- Scalene compartment — the median nerve's parent roots (C6, C7) pass through the scalene triangle, where fascial tightness can create low-grade neural tension
- Costoclavicular space — the brachial plexus passes between the clavicle and first rib, a common site of restriction
- Pectoralis minor — the nerve bundle dips under pectoralis minor at the coracoid; fascial densification here affects the entire downstream neural environment
- Bicipital aponeurosis (lacertus fibrosus) — the antebrachial fascia of the forearm connects to this structure; fascial loading here influences the forearm flexor compartment
- Pronator teres — the median nerve passes between the two heads of pronator teres, a common site of entrapment and sensitisation
- Transverse carpal ligament — the terminal compression site
This matters clinically because of what is sometimes called the double-crush concept: a nerve that is already sensitised by proximal fascial restriction is more vulnerable to compression distally. Treating only the wrist without assessing this upstream environment often addresses the symptom site but not the mechanical context that produced it.
This is not theoretical. The manual therapy protocol used in the Fernández-de-las-Peñas 2017 RCT — which showed equivalence to surgery at 12 months — specifically targeted the scalene, costoclavicle space, pectoralis minor, bicipital aponeurosis, pronator teres, transverse carpal ligament, and palmar aponeurosis in sequence. That is a direct description of upper limb chain assessment. The treatment site is not just the wrist; it is the entire fascial environment through which the nerve travels.
What Does the Research Say?
Clinical practice guidelines recommend manual therapy as part of conservative management for CTS. The JOSPT Clinical Practice Guidelines for Carpal Tunnel Syndrome (Erickson et al., 2019) — the current gold-standard CPG for this condition — include manual therapy and neural mobilisation among recommended intervention categories, alongside splinting and exercise-based approaches. The guideline emphasises a multimodal assessment framework including neurodynamic testing of the upper limb to identify proximal contributors to symptoms. [1]
Manual therapy has been shown to produce outcomes equivalent to surgery at 12 months. A randomised controlled trial by Fernández-de-las-Peñas et al. (2017) compared manual therapy (targeting the full upper limb fascial chain from scalene to palm) with surgical carpal tunnel release in 100 women with CTS. Manual therapy produced significantly better outcomes at one month for self-reported function and pinch grip force. At 3, 6, and 12 months, both groups showed equivalent improvement in function, symptom severity, and grip strength. This is level 1b evidence supporting conservative management as a primary, not secondary, option. [2]
Fascial densification can entrap peripheral nerves independent of bony compression. Research into fascial entrapment neuropathy demonstrates that thickening of the loose connective tissue layer surrounding peripheral nerves — detectable on ultrasound elastography — can impair neural mobility and vascular supply without structural narrowing of the bony canal. This model, developed within fascial anatomy research, applies directly to CTS and helps explain why some people respond to soft tissue approaches even when bony tunnel dimensions appear normal. [3]
How We Approach Carpal Tunnel Syndrome
Our assessment does not start at the wrist. We evaluate the full upper limb chain — cervical spine, scalene compartment, thoracic outlet, pectoralis minor, forearm flexor compartment, and the wrist — to identify where fascial densification and restricted neural mobility are most prominent. Movement assessment looks at how posture, breathing pattern, and shoulder mechanics are influencing loading on the nerve's course.
Treatment is directed at the tissues that appear most restricted along the chain, using Fascial Manipulation to restore mobility at identified centres of coordination. We also address movement patterns — wrist position at the desk, grip strategy under load, neck and shoulder posture during sustained work — that continue to load the neural container once treatment ends.
The goal is to reduce the cumulative load on the median nerve by improving the mechanical environment it travels through, not only at the wrist but along its entire course.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Modify your wrist position at the keyboard.
The wrist should be neutral — not flexed downward or extended upward — during keyboard and mouse use. A padded wrist rest used to hold the wrist in position (rather than to rest on between keystrokes) often makes things worse. A flat surface with the wrist held neutrally by the forearm muscles is preferred.
2. Try a night splint.
Many people find that symptoms are worst at night because the wrist falls into flexion during sleep. A neutral-position wrist splint worn during sleep can reduce nocturnal symptoms significantly. These are available from most pharmacies and do not require a prescription.
3. Perform nerve gliding exercises.
Gentle nerve gliding exercises — where the wrist and fingers are taken through a specific sequence of positions — aim to restore mobility along the median nerve's course. These are low-load, suitable for most presentations, and are included in the JOSPT Clinical Practice Guidelines as a recommended exercise approach. A physiotherapist or chiropractor can guide the appropriate technique for your presentation.
4. Assess your neck and shoulder posture.
Sustained forward head posture and rounded shoulder position load the proximal fascial environment through which the median nerve travels. Regular breaks from sustained desk posture — and attention to neck and shoulder position — can reduce the cumulative neural load that contributes to symptoms.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
Carpal tunnel syndrome develops within a fascial chain that extends from the thoracic outlet through the forearm to the carpal tunnel — compression at multiple points along this chain can compound nerve irritation. This pillar article maps the full upper limb fascial context.
Read Article →Breathing pattern dysfunction loads the scalenes and thoracic inlet structures chronically — contributing to the double-crush phenomenon where the median nerve is sensitised proximally before it reaches the carpal tunnel. This article explains the breathing-nerve connection relevant to CTS.
Read Article →References
- PubMed Erickson M, Lawrence M, Stegink Jansen CW, Coker D, Amadio P, Cleary C (2019). Hand Pain and Sensory Deficits: Carpal Tunnel Syndrome — Clinical Practice Guidelines. Journal of Orthopaedic & Sports Physical Therapy, 49(5), CPG1–CPG85.
- PubMed Fernández-de-las-Peñas C, Cleland J, Palacios-Ceña M, Fuensalida-Novo S, Pareja JA, Alonso-Blanco C (2017). The Effectiveness of Manual Therapy Versus Surgery on Self-reported Function, Cervical Range of Motion, and Pinch Grip Force in Carpal Tunnel Syndrome: A Randomized Clinical Trial. Journal of Orthopaedic & Sports Physical Therapy, 47(3), 151–161.
- PubMed Stecco C (2019). Fascial entrapment neuropathy. Clinical Anatomy, 32(7), 884–891.