 By Dr Steven Hewitt — Chiropractor · AHPRA: CHI0001115420 · 9 June 2026
By Dr Steven Hewitt — Chiropractor · AHPRA: CHI0001115420 · 9 June 2026
Getting the distinction right changes what treatment actually looks like — and why generic “glute exercises” so often produce frustration rather than results.
Category: Clinical Education · Related: Hip Pain · Low Back Pain · Knee Pain · The Fascial Approach to Hip Pain · The Fascial Approach to Lower Back Pain · The Fascial Approach to Knee Pain
Why the back that aches after standing is often a glute problem in disguise
Gluteal dysfunction rarely announces itself as “weak glutes.” It announces itself as pain somewhere else — and lower back pain is the most common of those somewhere elses.
Here is what the research tells us. When previously pain-free people are asked to stand still for two hours, a striking proportion develop low back pain — and those who do share a consistent neuromuscular signature before the pain even starts. Their gluteus medius muscles — on the outer side of each hip — begin co-contracting: both sides bracing simultaneously, rather than the normal pattern of alternating control. A 2008 study by Nelson-Wong and Callaghan found this bilateral gluteus medius co-activation pattern correctly identified 76% of who would develop pain, with a sensitivity of 87%. [1]
The more important finding came six years later from the same research group: people who developed transient pain during standing were roughly three times more likely to experience a genuine clinical episode of low back pain over the following two years, compared to those who remained pain-free. [2] This shifts the story from correlation to prediction — the gluteal pattern appears to precede the pain, not merely accompany it.
Marshall and colleagues extended the finding: those who developed pain during prolonged standing also had lower side-bridge endurance and higher bilateral gluteus medius co-activation — the endurance deficit measurable before the pain appeared. [3] Cooper and colleagues confirmed the clinical prevalence: in a sample of 150 people with chronic non-specific low back pain compared to 75 matched controls, gluteus medius weakness was significantly more common in the pain group, and was a predictor of LBP in regression analysis. [4]
When the gluteus medius is unable to maintain alternating pelvic control during standing and walking, the load is distributed differently — more compression, more shear, less stability. The back compensates. The back, eventually, complains.
Lateral hip pain — why “trochanteric bursitis” is usually the wrong label
Pain on the outside of the hip, right over the bony prominence, worse when lying on that side, climbing stairs, or sitting with the legs crossed. This presentation has been called “trochanteric bursitis” for decades, and that label has driven a great deal of management that does not address the actual pathology.
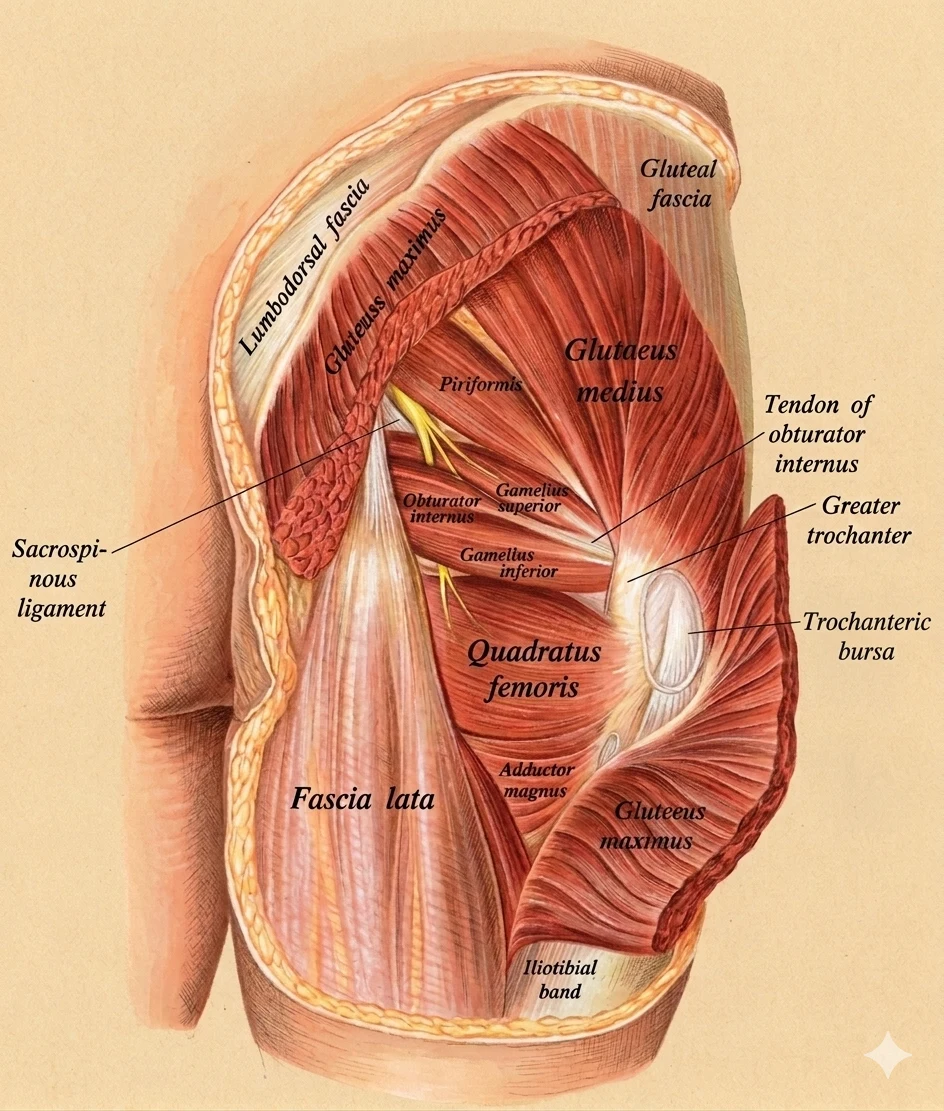
We now understand that the overwhelming majority of lateral hip pain originates in the tendons of the gluteus medius and gluteus minimus where they insert onto the greater trochanter. [5] The bursa is usually a secondary finding — irritated by proximity to the pathological tendon, not the primary driver of the problem.
The distinction matters for management. Tendinopathy is driven by mechanical load — specifically, by the combination of excessive tension and compression. Hip adduction (the hip falling inward, cross-legged sitting, standing with the weight entirely on one leg) compresses the gluteal tendons against the greater trochanter. The first priority in management is not to stretch or inject, but to understand and modify the positions and loads that drive that compression.
The LEAP trial — the first high-quality randomised controlled trial in this area, published in the BMJ in 2018 — found that an education-plus-load-management program was superior to corticosteroid injection and to a wait-and-see approach, with the advantage most apparent at longer follow-up. [6] The practical upshot: the most important early intervention is not a procedure or an exercise program, but an understanding of which positions to avoid and why. → Gluteal Tendinopathy
The knee that caves — when the hip is where the fault lies
Runner’s knee, patellofemoral pain, anterior knee pain — whichever label is used, the pattern is familiar. Pain around or behind the kneecap, often worse on stairs, hills, or after prolonged sitting.
Research has consistently identified a proximal contributor. When the gluteus medius is unable to adequately control the femur in the frontal plane, the knee drifts inward on every step — particularly under load, at the moment the foot hits the ground. This dynamic valgus pattern increases the forces acting on the patellofemoral joint and concentrates load in ways the joint is not designed to sustain over thousands of repetitions.
Studies have also found that the gluteal deficit in patellofemoral pain is not simply one of strength. It is frequently one of timing. A systematic review found that people with patellofemoral pain demonstrate delayed onset and shorter duration of gluteus medius activation during gait — the muscle fires later and switches off sooner, in the moments when femoral control is most needed. [7] Strengthening the muscle on a treatment table may not address a problem that is fundamentally about when and how it recruits during movement.
Targeted hip strengthening has been shown to improve pain and function in patellofemoral pain. [8] The honest caveat is that improving strength and improving kinematics are not always the same outcome — several studies have found that symptom improvement precedes or occurs without measurable changes in movement patterns. Where the movement fault itself is the primary target, specific gait or movement retraining may need to be part of the plan.
Real-time gait retraining has demonstrated meaningful improvements in both pain and hip kinematics in runners with patellofemoral pain. In one study, targeted feedback of hip adduction during running produced a 23% reduction in peak hip adduction, a 86% reduction in pain, and an 18–20% reduction in impact loading rates — with changes persisting at one-month follow-up. [9] → Patellofemoral Pain Syndrome
What “lazy glutes” actually is — four measurable things, not one
Here is where the “gluteal amnesia” framing breaks down — not because the glutes are fine, but because it conflates at least four separate, measurable problems.
Morphological change — the muscle physically alters. MRI studies in people with chronic low back pain and hip osteoarthritis demonstrate measurable gluteal atrophy and fatty infiltration. In hip osteoarthritis, wasting is most pronounced in the muscles that should be doing the most work — the gluteus medius and the deep abductors. [10] Progressive resistance training has been shown to partially reverse this in hip OA populations. [11]
Activation amplitude and timing — the muscle fires late and briefly. This is the most clinically underappreciated layer. In many presentations, the issue is not that the muscle cannot generate force — it is that it fires too late and disengages too early. The window during which pelvic and femoral control is most demanded is exactly the window in which the muscle is least available. [7]
Altered corticomotor representation — the brain’s connection to the muscle changes. This is where the “amnesia” metaphor gets closest to being accurate, while still being imprecise. Targeted gluteus maximus activation training has been shown to produce measurable changes in corticomotor excitability — the strength of the brain’s drive to the muscle — after as little as one week of activation work. [12] This provides a biological basis for “priming” or activation-focused work before loading. It is not placebo.
Functional consequence — the cascade of downstream effects. When the three layers above interact — degraded tissue, mistimed activation, weakened neural drive — the observable result is the hip that drops, the knee that caves, the lower back that compensates and eventually complains.
The reason generic “glute exercises” so often plateau is that they address one layer while ignoring the others. A structural deficit requires months of progressive loading. A timing deficit requires movement and coordination work. A neural drive deficit benefits from targeted activation before loading. Matching the intervention to the actual deficit is the difference between a program that works and one that frustrates.
Why the fascial system makes this a whole-body problem
There is a dimension to gluteal dysfunction that most “glute” content misses entirely — and it is the dimension that explains why a local muscle deficit can produce symptoms that appear nowhere near the hip.
The gluteus maximus does not operate as an isolated hip extensor. It is structurally woven into the thoracolumbar fascia — the broad connective-tissue sheet that spans the lower back. Its fibres originate in part from the thoracolumbar fascia itself, from the sacrum, the coccyx, and the sacrotuberous ligament. At the sacroiliac joint, the gluteus maximus functions as a compression mechanism — tightening the joint to create stability during load transfer. This is what researchers mean by “force closure” at the SIJ — an anatomical relationship confirmed in detail in cadaveric dissection. [13]
Most significantly, there is a diagonal sling: latissimus dorsi on one side, crossing through the thoracolumbar fascia, connecting to the gluteus maximus on the opposite side. This posterior oblique sling system is not a theoretical model — it has been demonstrated in living people. Researchers tensioning the latissimus dorsi on one side produced measurable changes in passive hip stiffness and resting position on the opposite side, transmitted across the body through the fascial system. [14] A 2025 study extended this finding clinically: people with chronic low back pain show reduced force transmission through this sling compared to pain-free controls — the mechanism itself appears to be impaired in the chronic pain population. [15]
This is why the fascial lens matters for gluteal assessment. A muscle this structurally integrated into the lumbopelvic system cannot underperform quietly. Its effects distribute — to the SIJ, to the lower back, to the opposite hip, and via the iliotibial band and fascia lata, to the knee. For a full anatomical overview of this connective-tissue context, see our review of the thoracolumbar fascia and the posterior chain.
A note on the evidence: the research supports the mechanical continuity of these connections and their clinical relevance in chronic LBP. The leap from demonstrated force transmission to whole-body “myofascial chain” maps involves more inference than evidence — the two are worth keeping separate in clinical thinking.
Training the glutes — matched to the problem, matched to the population
There is no single correct glute exercise. There is a logic for selection, and it depends on what the actual deficit is and what population is being treated.
The force-vector principle. Gluteus maximus EMG activity is highest near full hip extension and lowest in deep hip flexion — the relationship is reliable and well-established. This is why hip-thrust variations produce substantially greater gluteus maximus activation than squatting movements: the hip thrust loads the muscle at the position where it generates peak activity, while a squat loads it in deep flexion where it contributes least. A head-to-head comparison found mean upper gluteus maximus activation of 69.5% of maximum in the barbell hip thrust versus 29.4% in the back squat — large effect sizes across multiple outcome measures. [16]
The squat is a valuable exercise. The practical point is that if the goal is specifically to load the gluteus maximus through its full range, extension-biased loading is more effective than flexion-dominant loading.
Important: These figures come from acute EMG studies. High activation in a single session does not confirm greater hypertrophy or better functional transfer over time — no longitudinal training study has yet compared these outcomes directly between squatting and hip-thrust patterns. The acute data support the exercise selection logic; they do not prove superiority on clinical outcomes.
For the lateral stabilisers — gluteus medius. The gluteus medius is a frontal-plane stabiliser. Exercises that require resisting hip drop and controlling the pelvis under single-leg load — single-leg standing, lateral band work, split-stance movements — more specifically challenge its stabilising role than bilateral exercises do.
By clinical presentation:
Chronic low back pain: Gluteus maximus and medius strengthening within a broader movement-control program. The posterior oblique sling rationale supports integrating some lat and cross-body loading — not as a gimmick, but because the system that requires rehabilitation spans the whole chain.
Lateral hip pain / GTPS: Staged load management guided by the LEAP protocol. [6] The priority is reducing compressive loads on the tendon — avoid hip adduction positions, avoid cross-legged sitting, avoid aggressive ITB or adductor stretching — before progressing tensile loading. Aggressive strengthening into a reactive tendinopathy worsens it.
Patellofemoral pain: Hip abductor and external rotator strengthening to improve frontal-plane control. [8] Be clear that stronger glutes usually mean less pain — but “less pain” and “better movement pattern” do not always arrive together. Improving load capacity does not necessarily in and of itself correct movement patterns. Research on gait retraining for runners has demonstrated positive changes in the kinematic parameters associated with patellofemoral pain independent of strength gains.
Hip osteoarthritis: Progressive, extension-biased strengthening to counter the selective extensor and abductor wasting. [11] There is a case for beginning this work early, given the bidirectional relationship between muscle quality and joint loading.
What this means for you
If you’ve been told you have “lazy glutes” and a few exercises haven’t changed much, the most likely explanation is not that you haven’t tried hard enough — it is that strength work alone is targeting one layer of a multi-layered problem. Pain and function improvements are realistic aims. Whether your movement pattern changes is a separate question with a separate intervention.
If you have persistent lower back pain and nobody has assessed how your hip stabilisers are working during standing and single-leg loading, that is a gap worth addressing. The research suggests it is one of the more predictive factors for who will continue to have problems and who will not. [1, 2]
If you have lateral hip pain and have been told you have bursitis, the more likely finding is tendinopathy of the gluteus medius or minimus insertion. Management should be directed at load, not at the bursa. What you do in the short term — particularly avoiding the compressive positions — matters as much as what exercise you add. [5, 6]
If your knee pain is worse on stairs and running, and strength training alone hasn’t resolved it, consider whether the problem is timing and movement rather than strength. Real-time gait retraining specifically targeting the mechanics during running has produced meaningful improvements in both pain and loading variables. [9]
Want to understand what’s actually driving your presentation?
Book Online — available 24/7
Call Now — speak with our team
Free 2-Week Rehab Program — request your copy
References
- PubMed Nelson-Wong E, Gregory D, Winter D, Callaghan JP (2008). Gluteus medius muscle activation patterns as a predictor of low back pain during standing. Clinical Biomechanics, 23(5), 545–553. [Paper 108]
- PubMed Nelson-Wong E, Callaghan JP (2014). Transient low back pain development during standing predicts future clinical low back pain in previously asymptomatic individuals. Spine, 39(6), E379–E383. [Paper 350]
- PubMed Marshall PW, Patel H, Callaghan JP (2011). Gluteus medius strength, endurance, and co-activation in the development of low back pain during prolonged standing. Human Movement Science, 30(1), 63–73. [Paper 109]
- PubMed Cooper NA, Scavo KM, Strickland KJ, Tipayamongkol N, Nicholson JD, Bewyer DC, Sluka KA (2016). Prevalence of gluteus medius weakness in people with chronic low back pain compared to healthy controls. European Spine Journal, 25(4), 1258–1265. [Paper 111]
- PubMed Grimaldi A, Mellor R, Hodges P, Bennell K, Wajswelner H, Vicenzino B (2015). Gluteal tendinopathy: a review of mechanisms, assessment and management. Sports Medicine, 45(8), 1107–1119. [Paper 351]
- PubMed Mellor R, Bennell K, Grimaldi A, Nicolson P, Kasza J, Hodges P, Wajswelner H, Vicenzino B (2018). Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy. BMJ, 361, k1662. [Paper 136]
- PubMed Barton CJ, Lack S, Malliaras P, Morrissey D (2013). Gluteal muscle activity and patellofemoral pain syndrome: a systematic review. British Journal of Sports Medicine, 47(4), 207–214. [Paper 352]
- PubMed Khayambashi K, Mohammadkhani Z, Ghaznavi K, Lyle MA, Powers CM (2012). The effects of isolated hip abductor and external rotator muscle strengthening on pain, health status, and hip strength in females with patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy, 42(1), 22–29. [Paper 353]
- PubMed Noehren B, Scholz J, Davis I (2011). The effect of real-time gait retraining on hip kinematics, pain and function in subjects with patellofemoral pain syndrome. British Journal of Sports Medicine, 45(9), 691–696. [Paper 360]
- PubMed Grimaldi A, Richardson C, Stanton W, Durbridge G, Donnelly W, Hides J (2009). The association between degenerative hip joint pathology and size of the gluteus medius, gluteus minimus and piriformis muscles. Manual Therapy, 14(6), 605–610. [Paper 354]
- PubMed Rostron ZPJ, Zacharias A, Semciw AI, Green RA, Pizzari T (2022). Effects of a targeted resistance intervention compared to a sham intervention on gluteal muscle hypertrophy, fatty infiltration and strength in people with hip osteoarthritis. BMC Musculoskeletal Disorders, 23(1), 944. [Paper 359]
- PubMed Fisher BE, Southam AC, Kuo YL, Lee YY, Powers CM (2016). Evidence of altered corticomotor excitability following targeted activation of gluteus maximus training in healthy individuals. Neuroreport, 27(6), 415–421. [Paper 355]
- PubMed Barker PJ, Hapuarachchi KS, Ross JA, Sambaiew E, Ranger TA, Briggs CA (2014). Anatomy and biomechanics of gluteus maximus and the thoracolumbar fascia at the sacroiliac joint. Clinical Anatomy, 27(2), 234–240. [Paper 356]
- PubMed Carvalhais VO, Ocarino JM, Araújo VL, Souza TR, Silva PLP, Fonseca ST (2013). Myofascial force transmission between the latissimus dorsi and gluteus maximus muscles: an in vivo experiment. Journal of Biomechanics, 46(5), 1003–1007. [Paper 98]
- PubMed Procópio PRS, Pinto RZ, Murta BAJ, et al. (2025). Individuals with chronic low back pain have reduced myofascial force transmission between latissimus dorsi and contralateral gluteus maximus muscles. Journal of Biomechanics, 190, 112850. [Paper 357]
- PubMed Contreras B, Vigotsky AD, Schoenfeld BJ, Beardsley C, Cronin J (2015). A comparison of gluteus maximus, biceps femoris, and vastus lateralis electromyographic activity in the back squat and barbell hip thrust exercises. Journal of Applied Biomechanics, 31(6), 452–458. [Paper 358]
Please note: This post is intended for educational purposes only and does not constitute clinical advice. Individual presentations vary significantly. Please consult a registered health practitioner for advice about your specific condition.