 By Dr Steven Hewitt — Chiropractor · AHPRA: CHI0001115420 · 22 May 2026 · ~7 min read
By Dr Steven Hewitt — Chiropractor · AHPRA: CHI0001115420 · 22 May 2026 · ~7 min read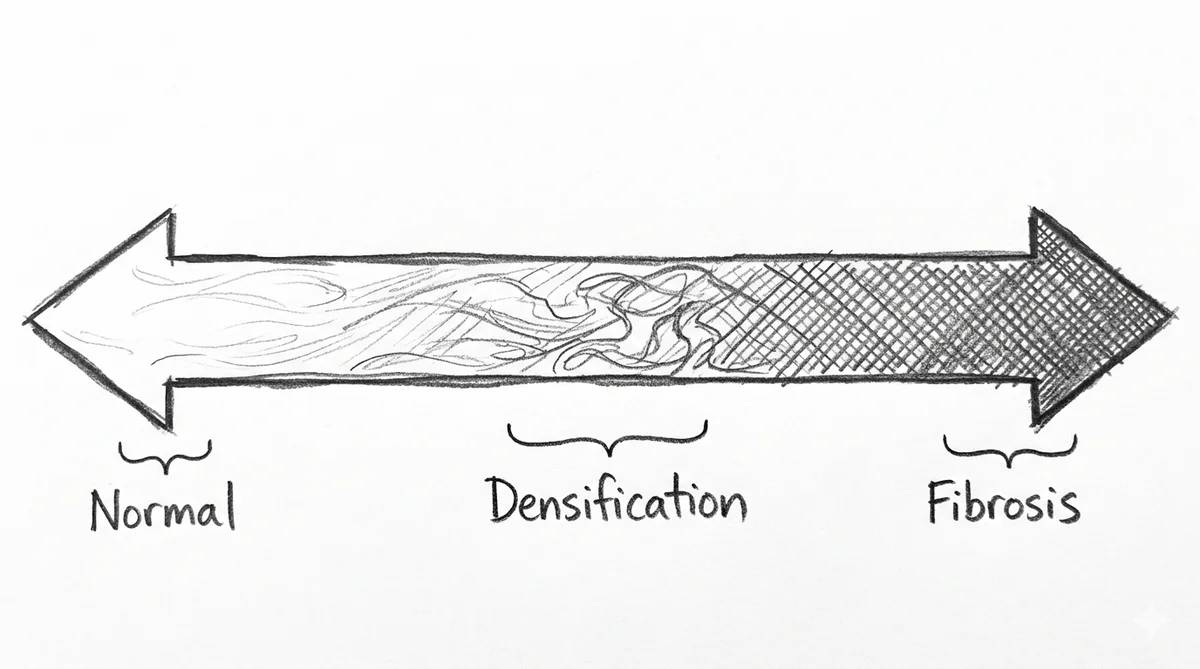
Most people who have been to a chiropractor or physiotherapist have heard something along the lines of: your muscles are tight, your fascia is restricted, the tissue isn’t moving the way it should. These are descriptions of something that is, in principle, reversible — a change in the mechanical state of the connective tissue that can be addressed with treatment, movement, and load management.
But there is a harder question behind that clinical picture, and the research is only beginning to work through it. Does fascial dysfunction, left unaddressed over time, progress? Is there a point at which what starts as a functional, reversible change becomes something more structural — and more difficult to reverse?
The honest answer is that we do not yet know. What the research does offer, however, is a biologically plausible picture of what that progression might look like, and some evidence from the structural end of the spectrum that suggests the question is worth taking seriously.
What densification actually is
To understand the question, it helps to be precise about the starting point.
Fascia — particularly the deep fascia that encloses and separates muscles — is not a static, passive wrapping. It is a living tissue with its own cellular biology, and one of the key molecules in that biology is hyaluronic acid (HA). HA is produced by specialised cells in the inner layer of the deep fascia called fasciacytes, and its job is to maintain the fluid environment of the loose connective tissue between fascial layers — the layer that allows one plane of tissue to glide over another. [1]
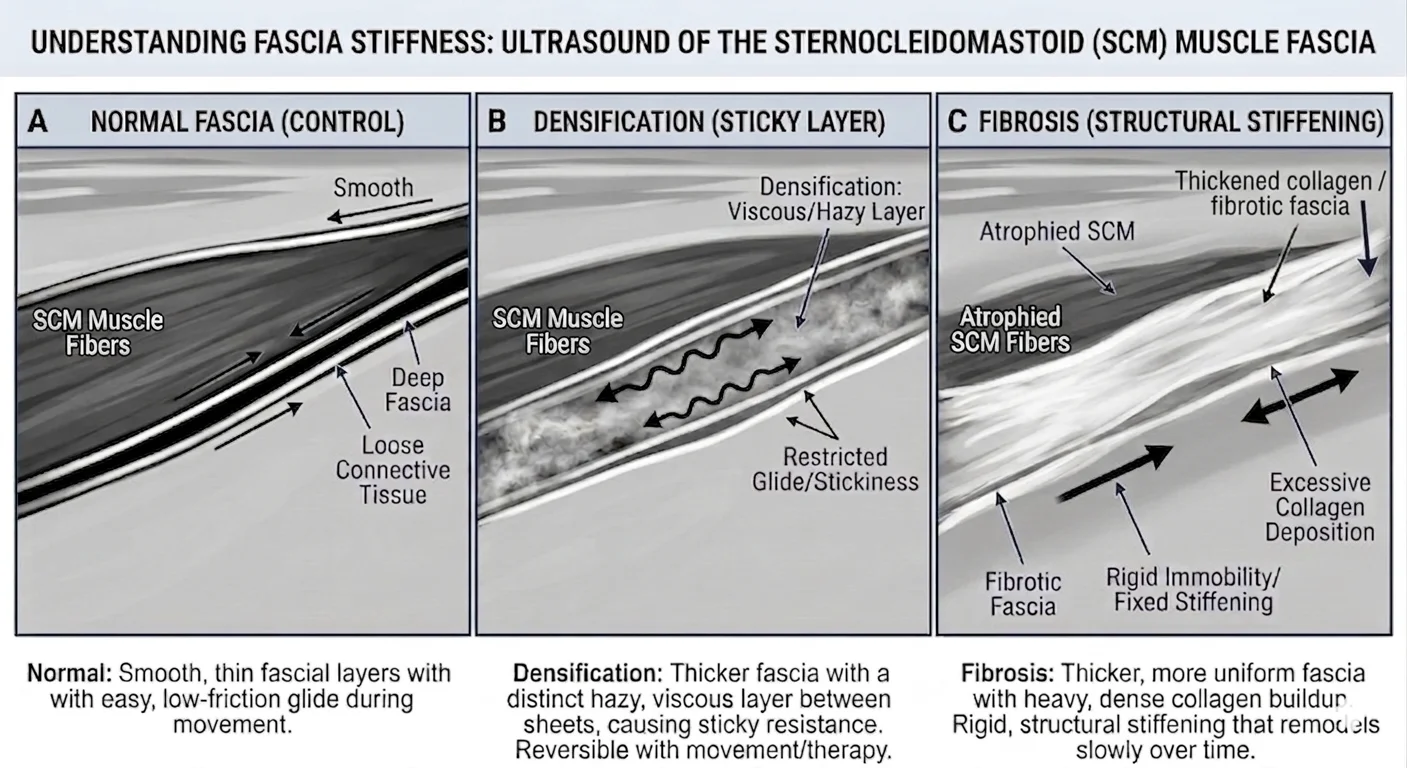
When this system is working normally, the HA remains in a fluid, low-viscosity state. The layers can glide freely; muscles move independently of each other; the mechanoreceptors embedded in the fascial tissue receive appropriate sensory input. When HA becomes aggregated — through sustained mechanical load, altered movement patterns, sustained posture, or local metabolic stress — its viscosity increases. It shifts from a sol (fluid) state to a gel (densified) state. The layers no longer glide as freely. Pavan and colleagues describe this as fascial densification: a change in the physical state of the ground substance, distinct from fibrosis, and in principle reversible. [2]
The molecular machinery underlying this shift has been mapped in a 2025 review by Kirkness and Scarlata, who propose the Ca²⁺–HA (CHA) axis as a unified mechanotransduction framework. [9] Mechanical force activates calcium channels (Piezo1, TRPV4, P2Y2) at the fasciacyte membrane, driving HAS2-mediated HA synthesis that peaks four to six hours post-stimulus. The molecular weight of synthesised HA determines the biological outcome: high-molecular-weight HA binds CD44 receptors to restore homeostasis (a “Quiet” state); low-molecular-weight fragments bind RHAMM receptors, amplifying pro-remodelling signalling (a “Riot” state). In healthy, normally loaded tissue, the system oscillates between these states to maintain ECM homeostasis. Under chronic or excessive mechanical stress, the balance can shift toward a sustained Riot state — laying the groundwork for the structural changes further along the continuum.
The reversibility is important. This is not scar tissue. The collagen fibre architecture does not change in simple densification. There is no permanent structural alteration. What has changed is the fluid environment — and restoring that environment, through movement, through load, through the kind of deep localised friction used in manual therapy, is biologically plausible as a mechanism of change. [3]
Where the biology gets more complicated
The clean distinction between densification and fibrosis is clinically useful, but it may not be the full picture.
Willard and colleagues, in their 2012 review of thoracolumbar fascia anatomy and function, described a finding that suggests the story does not always stop at reversible densification. [4] In people with chronic low back pain, the TLF can develop a pattern of tissue stiffening that resembles — both histologically and clinically — the presentation seen in frozen shoulder. This stiffening is associated with the activity of myofibroblasts: cells that occupy the fascial tissue and generate persistent contractile tension through a mechanism involving TGF-β1. Under sustained mechanical and chemical stimulus, fibroblasts in the connective tissue can differentiate into myofibroblasts, which maintain chronic fascial tension without direct neural drive. The result is a fascial environment that has moved beyond the simple sol→gel shift in HA viscosity — it has acquired a cellular component that sustains the restriction from within.
This is not the same as frank fibrosis. But it represents a middle ground that is meaningfully different from simple densification, and potentially more resistant to reversal.
The imaging literature is beginning to detect this structural middle ground non-invasively. Pirri and colleagues (2023) used ultrasound to measure the thickness of the thoracolumbar fascia in people with chronic non-specific low back pain and found it was significantly greater bilaterally compared with healthy controls — a finding consistent with the fascial thickening model and detectable without surgical exposure. [5] Their 2024 systematic review of TLF ultrasound studies confirmed that both B-mode and elastography techniques show altered fascial thickness and stiffness in the LBP population, and that these measurements are reliable and valid enough to use clinically. [6]
The cellular mechanism driving this middle-ground transition has been described more precisely by Kodama and colleagues (2023). [10] Fascial fibroblasts exposed to repeated mechanical stress undergo a stepwise transformation: first to proto-myofibroblasts (characterised by actin stress fibres), then to mature myofibroblasts that form fibronectin bridges and maintain chronic contractile force via TGF-β1 — independent of any neural drive. Two variables that modify the likelihood and pace of this transition are clinically relevant: ageing, which is associated with progressive lumbar fascial thickening (+40 to 77% in older cohorts compared with younger adults) even as lower limb fascia tends to thin; and estrogen, where receptor β (Erβ) activity normally inhibits TGF-β expression and the fibroblast-to-myofibroblast conversion, making prolonged estrogen deficiency a potential biological accelerant of fibrotic progression in the posterior fascial chain.
Pirri and colleagues (2025), in a narrative review examining fascia’s role in complex regional pain syndrome, trace the downstream consequences of the sustained inflammatory-fibrotic cycle. [11] Persistent elevation of pro-inflammatory cytokines — IL-1, IL-6, and TNF-α — drives excess ECM deposition and fibrosis, restricts mobility, and generates mechanical pain that in turn perpetuates the cycle. The thoracolumbar fascia, with a nociceptive fibre density of 9.01% of cross-sectional area — the highest of any fascia studied — is particularly capable of sustaining peripheral and, over time, central sensitisation once this cycle is established. The picture that emerges is not a series of disconnected events but a coherent, biologically plausible pathway: HA state change (CHA axis) → myofibroblast activation (TGF-β1) → structural thickening (ultrasound-detectable) → cytokine-driven fibrosis → nociceptor sensitisation.
So at the functional level, you have reversible HA densification. At the structural level, you have measurable TLF thickening and altered stiffness. In between, there is a biologically plausible myofibroblast-driven mechanism that may explain how one transitions to the other over time — although no prospective study has followed people from early densification through to structural fascial change, so that specific progression has not been confirmed.
The far end of the spectrum: what surgical studies show
The most graphic illustration of what structural fascial pathology can look like comes from the surgical literature — and one study in particular brings it into sharp relief, even if the clinical context is far removed from everyday musculoskeletal care.
Gfrerer and colleagues (2020) reported on 92 patients who underwent surgical decompression of the greater occipital nerve (GON) for intractable migraine and chronic headache — cases that had failed conservative management and were being considered for nerve surgery. [7] The cohort had a mean age of 44.8 years at the time of surgery, with a mean age at migraine onset of 22.9 years — implying an average of roughly 22 years between the start of symptoms and the point at which surgery was considered. What the surgeons found when they got to the tissue was striking: 94% of patients had trapezius fascia that was thicker than 3 mm and described as fibrotic at the time of surgery. To put that in context: a companion ultrasound study by the same research group measured trapezius fascia thickness at the same anatomical site in matched healthy controls and found a mean of 0.9 mm (SD 0.23 mm, maximum 1.2 mm). [8] A surgical finding exceeding 3 mm represents more than three times the mean healthy tissue thickness — not subtle thickening, but a substantial structural alteration. In 30% of cases, the GON was found to be encased in fibrotic tissue at the muscle-fascia interface.
This is not a study about fascial dysfunction in the ordinary sense. These are patients at the far end of the severity spectrum, treated with a procedure that most people with headache will never need. But the structural finding is significant: the fascia of the posterior cervical and suboccipital region, in a substantial proportion of this population, had crossed from altered mechanical state to frank structural fibrosis — and that fibrosis was directly impinging on a nerve pathway known to be involved in migraine.
The reported outcomes (75% improvement in Migraine Headache Index at follow-up) are outcomes from surgery — decompression — not from any conservative intervention. They are not being presented here as evidence that fascial treatment produces equivalent results. What the study does offer is a window into what the fascial environment can look like in a population with refractory headache, and why the quality of the fascial tissue in the cervical region is worth paying attention to well before that endpoint is reached.
What this means — and what it does not
It would be inaccurate to suggest that untreated fascial densification inevitably progresses to fibrosis. The research does not support that claim. There is no prospective study that has followed a cohort of people with early fascial densification and documented their progression to structural change. The pathway described above — densification → myofibroblast activation → structural thickening → fibrosis — is biologically plausible and supported by separate pieces of evidence, but it has not been confirmed as a direct causal chain.
What can be said is that these are not separate, unrelated phenomena. Densification, myofibroblast-driven stiffening, structural TLF thickening, and frank fascial fibrosis all involve the same tissue, the same cellular biology, and the same mechanical environment. The literature suggests they may occupy different points on a continuum rather than being categorically distinct conditions.
The implication for how we think about persistent or recurrent musculoskeletal presentations is modest but real. A fascial environment that has been under sustained altered mechanical load — from chronic posture, from restricted movement, from long-standing pain-driven compensation — is not necessarily in the same biological state as one that has been loaded functionally and moved freely. Assessing fascial tissue quality, and not just the muscles and joints around it, is a reasonable part of a thorough clinical evaluation. Whether restoring normal mechanical conditions earlier in the course of a presentation changes long-term outcomes is an important question that the research has not yet answered.
How we approach this clinically
The Fascial Manipulation framework assesses fascial tissue quality as part of every evaluation — palpating for densification (perceived as increased resistance or altered texture in the loose connective tissue), identifying which fascial sequences are altered, and determining whether the dysfunction is localised or part of a broader pattern. Treatment is directed at restoring the fluid environment of the densified tissue — using localised deep friction to generate heat and pressure that shifts HA toward a more fluid state. [3]
Whether that approach addresses the tissue at the reversible densification end of the spectrum or the structural end is something we cannot determine by palpation alone. But the biology of the system makes a compelling case for treating the functional end while it is still functional — before altered tissue mechanics have time to become structural alterations.
This is not a claim that treatment prevents fibrosis. We do not know that. It is an argument for taking the fascial tissue seriously as part of a complete clinical picture — which is what the research increasingly supports.
For more on the mechanism debate, see our article The Fascial Critics Have a Point. They’re Also Missing It. For the clinical application to headache and the posterior cervical fascial environment, see our page on Migraine — The Musculoskeletal Contribution.
Want to understand your own fascial health?
Call Now — speak with our team
Book Online — available 24/7
References
- PubMed Pratt RL. (2021). Hyaluronan and the fascial frontier. International Journal of Molecular Sciences, 22(12), 6368.
- PubMed Pavan PG, Stecco A, Stern R, Stecco C. (2014). Painful connections: densification versus fibrosis of fascia. Current Pain and Headache Reports, 18(8), 441.
- PubMed Ercole B, Stecco A, Day JA, Stecco C. (2010). How much time is required to modify a fascial fibrosis? Journal of Bodywork & Movement Therapies, 14(4), 318–325.
- PubMed Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. (2012). The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of Anatomy, 221(6), 507–536.
- DOI Pirri C et al. (2023). Ultrasound imaging of the thoracolumbar fascia in chronic non-specific low back pain. Diagnostics, 13, 1436.
- DOI Pirri C et al. (2024). Ultrasound imaging of the thoracolumbar fascia: a systematic review. Medicina, 60, 1090.
- PubMed Gfrerer L, Hansdorfer-Korzon R, Tsao L, Austen WG Jr. (2020). Trapezius fascia fibrosis in surgical migraine patients. Plastic and Reconstructive Surgery, 145(6), 1453–1460.
- PMC Chartier C, Gfrerer L, Austen WGG Jr. (2020). Ultrasonographic evidence of trapezius fascia thickening in patients undergoing trigger site deactivation surgery compared with healthy control. Plastic and Reconstructive Surgery — Global Open, 8(9 Suppl):25–26.
- DOI Kirkness KB, Scarlata S (2025). Understanding fascial tissue on the molecular level — how its unique properties enable adaptation or dysfunction. International Journal of Molecular Sciences, 27, 160.
- DOI Kodama Y, Masuda S, Ohmori T, Kanamaru A, Tanaka M, Sakaguchi T, Nakagawa M (2023). Response to mechanical properties and physiological challenges of fascia: diagnosis and rehabilitative therapeutic intervention for myofascial system disorders. Bioengineering, 10, 474.
- DOI Pirri C, Pirri N, Petrelli L, Fede C, De Caro R, Stecco C (2025). An emerging perspective on the role of fascia in complex regional pain syndrome: a narrative review. International Journal of Molecular Sciences, 26, 2826.
Please note: This post is intended for educational purposes only and does not constitute clinical advice. Individual presentations vary. Please consult a registered health practitioner for advice about your specific condition.