Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
What Is Achilles Tendinopathy?
The Achilles tendon is formed from the convergence of the gastrocnemius and soleus muscles (together, the triceps surae), inserting into the posterior surface of the calcaneus. It is the primary transmission structure for the propulsive force generated by the calf complex during walking, running, and jumping.
Achilles tendinopathy refers to a structural change in the tendon tissue in response to cumulative overload. It is not an inflammatory condition in the classical sense, but a biological and structural response to load that exceeds the tendon's adaptive capacity. Two anatomical locations are involved:
| Type | Location | Typical Presentation |
|---|---|---|
| Mid-portion tendinopathy | 2–7 cm above the calcaneal insertion | Pain and localised thickening in the tendon midsubstance |
| Insertional tendinopathy | At the calcaneal attachment | Pain directly at the heel bone; often worse with direct pressure (shoes, hard surfaces) |
The mid-portion type is most common in runners and younger-to-middle-aged active adults. Insertional tendinopathy is more common in older adults and is associated with calcaneal bone spurs and retrocalcaneal bursitis.
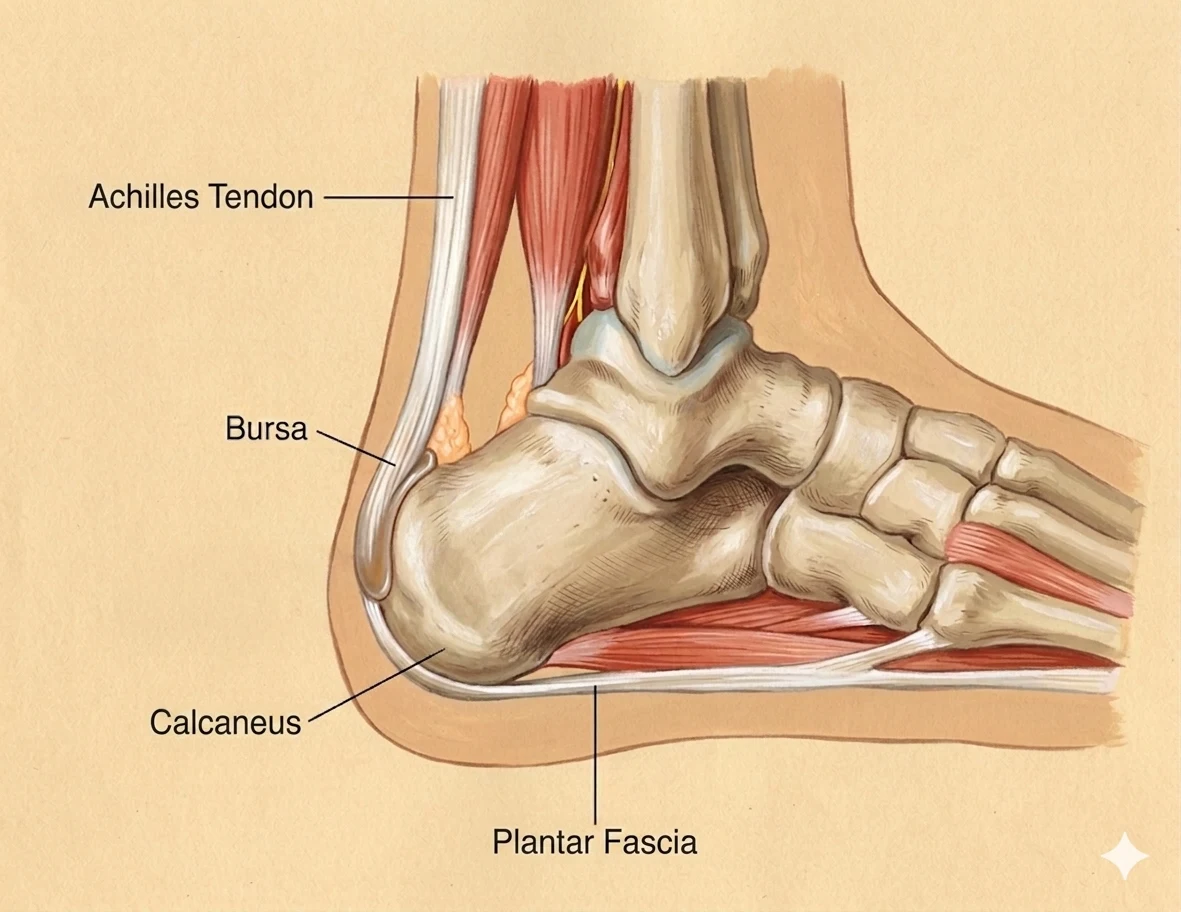
Lateral view of the heel — the Achilles tendon inserts into the posterior calcaneus with the retrocalcaneal bursa sitting between them. The plantar fascia originates from the inferior calcaneus and extends forward to the metatarsal heads. The two structures share calcaneal periosteum, which is why Achilles and plantar fascia pathology so often co-exist. Mid-portion tendinopathy occurs 2–7 cm above this insertion; insertional tendinopathy directly at the heel bone attachment.
Who Typically Experiences This?
Runners — especially those who have changed their training
A sudden increase in training volume, a change to a lower-drop shoe, a return to running after a break, or transitioning to harder surfaces are all common triggers. The Achilles tendon adapts to load — but the adaptation takes longer than the aerobic and muscular systems. When running volume outpaces tendon adaptation, the tissue begins to change.
Gym athletes and those who load the posterior chain heavily
Calf raises, plyometrics, Olympic lifting, and heavy compound movements all generate significant Achilles loading. When the posterior chain has restricted mobility upstream — tight hamstrings, limited hip extension, reduced thoracic mobility — the calf and Achilles absorb more than their share. We commonly see this in people who train consistently but without addressing the movement quality or fascial health of the broader chain.
The active person in their 40s and 50s
Achilles tendinopathy is very common in this demographic. Age-related changes in tendon biology — reduced collagen turnover, decreased water content, more brittle collagen crosslinks — mean the tendon's adaptive window narrows. This does not mean high load is contraindicated: progressive loading remains the primary evidence-informed approach. But it means load needs to be managed with more deliberate attention to recovery.
People with a history of plantar fasciopathy
The anatomical relationship between the Achilles paratenon and the plantar fascia means these two conditions frequently co-exist or occur sequentially. Research has demonstrated that plantar fascia thickness is significantly greater in people with Achilles tendon pathology, and the two structures share fascial continuity at the calcaneus [125]. Someone presenting with Achilles tendinopathy often has a plantar fascial system under similar mechanical stress.
Desk workers who run on weekends
The combination of prolonged sitting (which places the Achilles in a shortened, unloaded position for hours) followed by weekend running loads is a particularly common pattern. The tendon is not prepared for the demand asked of it at the weekend.
The Fascial Lens: Why We See This Differently
The Achilles is the bottom of the deep longitudinal sling
The Achilles tendon does not exist in anatomical isolation. It is the distal terminal of the deep longitudinal sling — the posterior chain that runs from the calcaneus upward through the calf, the peroneal complex, the biceps femoris and sacrotuberous ligament, and into the deep layer of the thoracolumbar fascia and the lumbar erector spinae. This chain distributes the forward shear forces generated at the lumbar spine with every step.
When any part of the chain is restricted — restricted ankle dorsiflexion, hamstring fascial tension, TLF densification, lumbar extension limitation — the load management function of the chain is compromised. The Achilles, as the terminal of the chain, absorbs a disproportionate share. This is why in-vivo research has demonstrated that ankle loading generates measurable soft tissue displacement in the dorsal thigh, confirming the mechanical integration of this chain in the living body [14]. The calf and Achilles are not doing their work independently.
The plantar fascia connection
Carla Stecco and colleagues' anatomical study demonstrated a direct tissue continuity between the Achilles paratenon and the plantar fascia, mediated through the periosteum of the calcaneus. They are not the same structure, but they are part of the same fascial system. The MRI data in that study showed that when the Achilles tendon shows signs of degeneration, the plantar fascia is on average 64% thicker than in people without Achilles pathology — a statistically highly significant difference (p<0.001) [125].
This means two things clinically. First, treating the Achilles without addressing the plantar fascial system on the same heel may be addressing half the picture. Second, and more importantly, the mechanical driver of pathology at the calcaneus is often not localised to the Achilles tendon or the plantar fascia — it is the broader fascial and kinetic chain environment that is loading both of them.
The paratenon — the fascial component of the Achilles
The Achilles tendon is surrounded by a paratenon — a sheath of connective tissue that allows the tendon to glide within its mechanical environment. The paratenon contains its own population of cells and is distinct from the tendon itself. In early Achilles tendinopathy, changes often occur first in the paratenon rather than the tendon proper — stiffening, losing its normal gliding capacity, contributing to the morning stiffness and warm-up period characteristic of this condition.
This paratenon is the tissue that directly connects to the plantar fascia at the calcaneus. Assessing and treating the fascial environment around the Achilles — not only the tendon — is central to how we approach this condition.
A continuum, not a fixed state
The pathology of Achilles tendinopathy exists on a spectrum. Early-stage reactive tendinopathy is a non-inflammatory proliferative response to overload — structurally, the collagen is intact and the changes may be fully reversible with appropriate load management. Mid-stage tendon dysrepair involves more structural disorganisation and increased vascular ingrowth. At the far end of the spectrum, degenerative change involves cell death and structural disruption that is less reversible.
Where on that spectrum a person sits has direct implications for how load should be managed — and is one reason that the same "Achilles problem" can have very different courses and respond differently to the same intervention [126].
What Does the Research Say?
Tendinopathy as a continuum of pathology
A landmark framework proposed that tendon pathology — including Achilles tendinopathy — exists on a spectrum from reactive change (reversible, non-inflammatory) through tendon dysrepair to degenerative pathology. This continuum model, now widely adopted in clinical practice, explains why presentation varies considerably and why treatment must be tailored to the stage of the pathology. Load management is the primary intervention at all stages, but the type and amount of appropriate load differs substantially between stages [126].
The Achilles–plantar fascia continuum at the calcaneus
Cadaveric dissection and MRI data confirmed that the Achilles paratenon and plantar fascia are continuous at the calcaneus. In patients with Achilles tendon degeneration, plantar fascia thickness averaged 3.43mm — compared to 2.09mm in those without Achilles pathology (p<0.001). There was a statistically significant correlation between Achilles paratenon thickness and plantar fascia thickness, confirming these structures share a mechanical and biological environment [125].
Myofascial force transmission through the deep longitudinal chain
In-vivo research demonstrated that passive ankle dorsiflexion produces measurable displacement of soft tissue in the dorsal thigh — providing direct evidence that the ankle and lower leg fascial system is mechanically integrated with the posterior chain above the knee [14]. When this chain is restricted, load at the Achilles is altered.
Fascial manipulation for musculoskeletal conditions
A systematic review of fascial manipulation for musculoskeletal pain and disability found consistent evidence for significant improvements in both pain and functional outcomes across multiple regions, including the lower limb [19].
How We Approach Achilles Tendinopathy
Establishing the stage
Our assessment begins with a detailed loading history — what changed before symptoms started, how irritable the tendon is currently (does it respond within 24 hours of loading?), and where on the continuum the presentation sits. This informs what type and amount of load is appropriate from the outset.
Fascial Manipulation assessment
We assess the fascial system of the calf, Achilles, posterior lower leg, foot, and the posterior chain above. Using the Stecco FM approach, we identify palpatory centres of coordination (CCs) where fascial densification is found — commonly in the calf, posterior lower leg, peroneal chain, and plantar fascia on the same side. Treatment at these points aims to restore fascial gliding and reduce the mechanical burden on the Achilles paratenon and tendon.
Progressive tendon loading
The evidence base for Achilles tendinopathy rehabilitation centres on progressive loading. The tendon remodels in response to appropriate mechanical input. We build a loading program from isometric holds (which provide analgesic effect in the reactive stage), through heavy slow resistance, to functional and sport-specific loading. The goal is to progressively expand the tendon's load tolerance within its current adaptive capacity.
Posterior chain assessment
We systematically assess ankle dorsiflexion range, hamstring and calf fascial mobility, hip extension, and — where relevant — thoracic and lumbopelvic mobility. Restrictions anywhere along the deep longitudinal sling are addressed in parallel with local tendon loading.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Load the tendon isometrically
For a painful, reactive Achilles, sustained calf raises held at the top position (isometric, 30–45 seconds, moderate to heavy load) can provide both analgesic effect and stimulus for tendon adaptation without the compressive and ballistic forces of dynamic loading. Five repetitions several times per day is a common starting point — but the load, position, and volume need to be appropriate for the current stage of your presentation.
2. Assess your ankle dorsiflexion
Stand facing a wall and step your foot forward until your toes are approximately 10–12cm from the wall. Keeping your heel on the ground, attempt to touch your knee to the wall. If you cannot do so without the heel rising, your ankle dorsiflexion is limited. Restricted dorsiflexion is a significant mechanical contributor to Achilles overloading. Calf stretching, ankle mobility drills, and fascial work through the posterior lower leg can gradually improve this range.
3. Don't make sudden changes to footwear or training surface
Transitioning to a lower-drop shoe, changing to harder running surfaces, or dramatically changing training volume are among the most common triggers for Achilles tendinopathy. If change is needed, it should be gradual — allowing the tendon time to adapt to the new mechanical environment.
4. Avoid complete rest
The Achilles tendon does not recover well with full rest. Deloading — reducing the most provocative activities while maintaining gentle movement and some degree of loading — is preferable to stopping entirely. The tendon requires mechanical input to stimulate the remodelling process that leads to recovery.
Take the Next Step
Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
Achilles tendinopathy sits within a fascial system that includes the plantar fascia, calcaneus, and posterior chain — load distribution through this system determines tendon stress. This pillar article maps the fascial relationships governing ankle and Achilles health.
Read Article →First MTP restriction forces the foot into supination during late stance, altering Achilles tendon load timing and direction. This article traces how a stiff big toe can drive compensatory strain up through the Achilles — a connection often missed in standard assessment.
Read Article →References
- PubMed Cook JL, Purdam CR (2009). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6), 409–416.
- PubMed Stecco C, Corradin M, Macchi V, et al. (2013). Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. Journal of Anatomy, 223(6), 665–676.
- PubMed Wilke J, et al. (2020). Ankle motion displaces soft tissue in the dorsal thigh — evidence for myofascial force transmission. Frontiers in Physiology, 11, 180.
- PubMed Arumugam A, et al. (2021). Effectiveness of fascial manipulation on pain and disability in musculoskeletal conditions: a systematic review. Journal of Bodywork and Movement Therapies, 25, 100–109.
- PubMed Van Wingerden JP, Vleeming A, Snijders CJ, Stoeckart R (1993). A functional-anatomical approach to the spine-pelvis mechanism: interaction between the biceps femoris muscle and the sacrotuberous ligament. European Spine Journal, 2(3), 140–144.