Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
What Is AC Joint Pain?
The acromioclavicular joint is a small synovial joint where the lateral end of the clavicle (collarbone) meets the acromion of the scapula (shoulder blade). It is stabilised by a layered system: the AC ligaments and joint capsule provide horizontal restraint, the coracoclavicular (CC) ligaments provide vertical restraint, and a fibrous sheet called the deltotrapezial fascia (DTF) — formed where the deltoid and trapezius muscles meet above the joint — contributes additional dynamic support [2, 3, 4, 5].
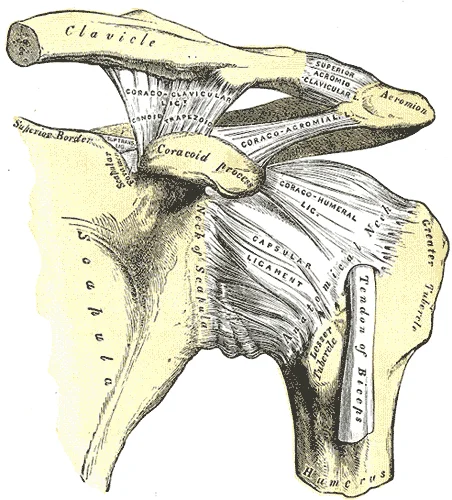
The left shoulder from the front — the acromioclavicular joint sits at the top, where the clavicle meets the acromion. The coracoclavicular ligaments run from the coracoid process up to the underside of the clavicle, providing vertical restraint. What this classical illustration cannot show is the deltotrapezial fascia — the fibrous sheet formed by the deltoid and trapezius muscles directly over this joint, which modern research has identified as a genuine dynamic stabiliser but which is largely absent from anatomy textbooks of this era. Illustration: Henry Vandyke Carter, Gray's Anatomy (1918) — public domain.
AC joint pain broadly falls into two clinical pictures, and distinguishing between them matters:
| Presentation | Typical cause | Typical management pathway |
|---|---|---|
| Acute AC joint sprain / separation | Direct fall onto the point of the shoulder, or a fall onto an outstretched arm; graded I–VI on the Rockwood classification by severity | Lower grades (I–II) usually managed conservatively; higher grades (especially IV–VI, where the clavicle is grossly displaced) usually require an orthopaedic surgical opinion |
| Chronic AC joint overload / osteoarthritis | Repeated compressive and shear loading — heavy bench pressing, dips, overhead work, or a history of an old, undertreated sprain | Usually managed conservatively; this is the more common presentation in an active gym-going population |
A structured diagnostic algorithm for shoulder pain identifies a useful clinical discriminator: pain reproduced by elevating the arm in the range of 60–120° is more typical of rotator cuff or subacromial pathology, whereas pain at the extremes of range — particularly horizontal (cross-body) adduction or pain past 120° of elevation — points more specifically to the AC joint [1]. A finger pointed precisely at the AC joint, rather than a palm placed broadly over the front of the shoulder, is also a useful clinical clue toward an AC-joint source [1].
Key facts
| Feature | Detail |
|---|---|
| Joint type | Small synovial joint, lateral clavicle to acromion |
| Primary static stabilisers | AC ligaments/capsule (horizontal), coracoclavicular ligaments (vertical) |
| Primary dynamic stabiliser | Deltotrapezial fascia (DTF) — common aponeurosis of deltoid and trapezius [3] |
| Typical pain location | Point-localised, directly over the joint |
| Typical aggravating movements | Cross-body (horizontal) adduction; end-range overhead elevation; direct pressure (lying on the side, seatbelt) |
| Distinguishing feature from rotator cuff pain | Pain at the extremes of range rather than the mid-range painful arc [1] |
Who Typically Experiences This?
The gym-goer with bench press or dip-related shoulder pain
Heavy horizontal pressing and dipping place the AC joint through repeated compressive and shear loading at the very end of the movement's range. In our clinical experience, this is one of the most common ways AC joint pain presents in an active population — a gradual ache that becomes a sharp, localised pain specifically at end range, rather than a single traumatic event. Because the pain can initially feel broadly "in the shoulder," the specific end-range and cross-body pattern that points to the AC joint is sometimes only identified once it is specifically assessed for.
The contact or collision sport athlete
Rugby, AFL, judo, and similar sports carry direct risk of falls onto the point of the shoulder or onto an outstretched arm — the classic mechanism for an acute AC joint sprain. The severity of these injuries varies enormously, from a mild Grade I sprain that settles within weeks to a high-grade separation with a visibly prominent clavicle that requires surgical assessment.
The desk worker or driver with an old, undertreated AC joint injury
A fall from years earlier — a bike accident, a ski fall, a minor car accident — that was never formally assessed can leave behind residual joint irritability or early osteoarthritic change at the AC joint. This often resurfaces later in life, sometimes provoked by a new but unrelated activity, with the person having forgotten the original injury was ever significant.
The overhead worker or tradesperson
Painters, plasterers, and other trades involving sustained overhead arm positions place repeated end-range load through the AC joint over a working day. This group often presents later, having attributed the discomfort to general shoulder fatigue rather than identifying the AC joint specifically.
The Fascial Lens: Why We See This Differently
The AC joint does not stabilise itself — the deltoid and trapezius do real mechanical work
For a long time, the biomechanical story of the AC joint was told almost entirely through its ligaments — the AC ligaments controlling horizontal movement, the CC ligaments controlling vertical movement. The deltotrapezial fascia was, until recently, largely absent from anatomy textbooks altogether. A 2020 anatomic study found a clear reason why: the DTF is a well-defined, robust fibrous structure in fresh tissue, but becomes almost invisible once standard preservation techniques (formalin, alcohol, Thiel fixation) are applied — which is very likely why generations of anatomists never identified it as a discrete structure, even though shoulder surgeons have operated on it for decades [3].
Once researchers began studying the DTF directly, a consistent picture emerged. Cadaveric studies isolating the deltoid and trapezius muscles — leaving the AC ligaments and capsule fully intact — found that cutting these muscles' attachments reduced the joint's resistance to rotation by approximately 10% in both directions, and that even a carefully performed surgical repair of these muscles could not fully restore the joint's original stability [4]. A separate study testing horizontal (front-to-back) stability specifically found that cutting the DTF significantly increased joint displacement, and that reconstructing it restored stability back to the level of the uninjured joint [5]. Detailed footprint-mapping work has also shown that the deltoid and trapezius are not simply muscles sitting near the AC joint capsule — they are anatomically continuous with it, blending directly into roughly 90% of the front of the joint capsule and a substantial portion of the back and top of the capsule [6]. Taken together, this body of work supports a joint that is actively held together by muscle and fascia, not just by its ligaments.
A comprehensive 2023 review of shoulder-girdle biomechanics puts this into an elegant mechanical framework. Because no muscle attaches to the collarbone in a way that can actively rotate it, the clavicle behaves as what the authors call an intercalated segment — a bone moved largely passively through its roughly 30° of rotation during arm elevation, dependent on the surrounding capsule, ligaments and fascia to control its position [12]. The same review describes how the deltoid and upper trapezius leave around 80% of the top of the outer collarbone as a "bare area" with no direct muscular attachment — and it is precisely this gap that the deltotrapezial fascia bridges, connecting the fascia of the two muscles and acting, in the authors' words, as a "dynamic sling" that both stabilises the shoulder girdle and dampens force transmission across the joint (they compare it to a dashpot — the damping element in a mechanical model) [12]. It is a vivid way of making the same point: the AC joint is not a rigid hinge held by ligaments alone, but a junction managed continuously by the surrounding myofascial envelope.
A note on what we observe clinically
In clinical practice, we commonly see AC joint–area pain provoked specifically at end-range positions — horizontal adduction or maximal humeral flexion — rather than through the joint's resting range. This pattern is consistent with a load-sharing problem at end range, rather than a purely local joint or ligamentous issue.
The posterior oblique sling and anterior oblique sling both cross the shoulder girdle and influence how load is distributed across the shoulder during these end-range movements [7, 8, 9, 10]. Our clinical observation is that addressing restriction within these myofascial slings — rather than treating the AC joint in isolation — is often associated with a reduction in this end-range pain.
It's important to be transparent about the evidence here: this specific clinical pattern and approach has not yet been studied in controlled trials, and we are not aware of published research testing whether fascial treatment changes AC joint load distribution or pain directly. What we can say is that the AC joint is anatomically and biomechanically connected to the surrounding myofascial system in ways that make this a plausible mechanism worth exploring [3, 6]. Given the low risk and low cost of this approach, we consider a trial of treatment directed at the relevant sling(s) a reasonable starting point for this presentation, alongside standard assessment to rule out higher-grade AC joint injury.
Why this matters for surgical decision-making too
The same research has a direct surgical implication, which is worth including because it illustrates how seriously this connective tissue is now being taken: studies have found that up to roughly 93% of patients requiring surgery for a complete acute AC joint dislocation have damage to the deltoid, trapezius, or both — and several research groups now argue that minimising surgical injury to these muscles, and properly repairing them when they are damaged, may improve outcomes after AC joint reconstruction [4, 5]. This is reinforced by biomechanical work on the reconstructions themselves: in one cadaveric study, when the AC capsule and deltotrapezial fascia were removed, rebuilding only the vertical (coracoclavicular) ligaments restored up-and-down stability but left the joint loose in the front-to-back direction — and even adding a suture directly across the joint did not recover horizontal stability, indicating that horizontal restraint depends on the capsule-and-fascia envelope rather than the vertical ligaments [11]. This is not something we perform ourselves — it is surgical context — but it reinforces that the muscle and fascia around the AC joint, not just the joint itself, is now considered clinically important.
What Does the Research Say?
The deltotrapezial fascia is a genuine structure with a fixation-related blind spot in anatomical science
An anatomic study of 11 cadaveric shoulders found the deltotrapezial fascia (DTF) — the fibrous sheet formed by the deltoid and trapezius above the AC joint — to be a clearly defined, measurable structure (mean thickness 1.7mm directly over the joint) in fresh tissue, but almost undetectable after standard fixation methods. This is likely why it has been absent from anatomy textbooks and the official anatomical naming register, despite being well recognised by shoulder surgeons [3].
Cutting the deltoid and trapezius measurably reduces AC joint rotational stability
A cadaveric biomechanical study isolating the deltoid and trapezius (with the AC ligaments and capsule left fully intact) found that combined injury to these muscles reduced the joint's resistance to rotation by approximately 9–10% in both directions, and that a careful anatomic surgical repair improved but did not fully restore this stability [4].
Reconstructing the deltotrapezial fascia restores horizontal joint stability in cadaveric testing
A separate cadaveric study using cyclic loading found that cutting the DTF significantly increased horizontal displacement of the joint, and that surgically reconstructing the DTF restored horizontal stability to a level not significantly different from the uninjured joint [5].
The deltoid and trapezius are anatomically continuous with the joint capsule, not simply adjacent to it
Detailed footprint-mapping of cadaveric shoulders found the deltoid muscle attaches to roughly 90% of the front portion of the AC joint capsule, and the trapezius attaches to a substantial portion of the back and top of the capsule — demonstrating direct anatomical continuity rather than the muscles and capsule being separate, simply neighbouring structures [6].
A combined injury to the AC ligaments and the DTF produces a small but measurable increase in joint movement
An earlier cadaveric study found that a combined lesion of the AC ligaments and the DTF produced a small but statistically significant increase in forward rotation and a tendency toward increased side-to-side movement of the clavicle, supporting the idea that the ligaments and the DTF work together rather than independently [2].
The clavicle is a passively controlled "intercalated segment" whose stability depends on the surrounding soft-tissue envelope
A 2023 review of shoulder-girdle biomechanics notes that no muscle inserts on the clavicle in a way that can actively produce its rotation during arm elevation — the bone is moved largely passively and held in position by its capsule, ligaments and the deltotrapezial fascia, which the review frames as a "dynamic sling" bridging the roughly 80% of the upper collarbone that has no direct muscular attachment. The review also summarises cadaveric data showing that complete loss of the AC capsule reduces the joint's resistance to backward rotation by around 94% — underlining how much of this joint's horizontal and rotational control lives in its soft-tissue envelope rather than its bony architecture [12].
Rebuilding the vertical ligaments alone does not restore horizontal stability
A cadaveric study comparing three surgical AC-joint stabilisation techniques found that reconstructing the coracoclavicular (vertical) ligaments restored up-and-down stability to normal, but none of the techniques — including one that added a suture directly across the joint — restored front-to-back (horizontal) stability while the AC capsule and deltotrapezial fascia remained unrepaired. This reinforces that horizontal stability at the AC joint is specifically a function of the capsule-and-fascia envelope [11].
A structured diagnostic approach helps separate AC joint pain from rotator cuff and other shoulder pathology
A published clinical diagnostic algorithm identifies pain at the extremes of shoulder movement — particularly cross-body adduction and elevation past 120° — together with point-specific (rather than broad) pain localisation, as useful discriminators between AC joint pathology and rotator cuff or subacromial pain [1].
How We Approach AC Joint Pain
Careful history and assessment first
Our assessment starts with the mechanism and pattern of onset — whether this is a recent traumatic injury or a gradually developing overuse pattern — together with movement testing to localise the pain specifically to the AC joint rather than the rotator cuff, biceps tendon, or referred cervical sources [1].
Recognising when this is outside our scope
Where the history or examination suggests a higher-grade AC joint separation — particularly visible deformity of the joint, significant trauma, or instability on examination — we refer for orthopaedic and imaging assessment before any other management is considered. AC joint injuries are graded by severity, and the higher grades are a surgical decision, not a conservative-care one.
Fascial and sling assessment for the overuse / chronic presentation
For the more common chronic or overuse presentation, we assess the myofascial slings that cross the shoulder girdle — particularly the posterior oblique and anterior oblique slings — for restrictions that may be altering how load is shared across the AC joint during end-range movement. As outlined above, this approach is grounded in plausible anatomical and biomechanical reasoning rather than AC-joint-specific clinical trial evidence, and we offer it as a considered trial of treatment rather than a guaranteed solution.
Load management
We assess which specific movements and positions provoke the joint — often a narrow, end-range pattern rather than the whole range of shoulder movement — and adjust training or work loading accordingly while the joint settles, rather than recommending blanket rest from all shoulder activity.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Identify your specific aggravating position
Notice whether your pain is provoked broadly through the middle of an overhead movement, or specifically at the very end of cross-body reaching or pressing. This distinction is a useful piece of information to bring to an assessment, as it helps differentiate an AC joint pattern from other shoulder presentations [1].
2. Temporarily modify, rather than avoid, end-range loading
If a specific position — the bottom of a dip, the top of a cross-body stretch, lying directly on that shoulder — consistently provokes the joint, reducing or modifying that specific position while maintaining general shoulder movement allows the joint to settle without full deconditioning.
3. Seek assessment promptly after a significant fall
A fall directly onto the point of the shoulder, with visible swelling, deformity, or an inability to use the arm normally, warrants prompt assessment rather than a "wait and see" approach — early grading of the injury guides whether conservative care or a surgical opinion is the appropriate next step.
4. Don't assume an old, forgotten injury is unrelated
If your AC joint pain has returned after years without symptoms, mention any old shoulder injury — even a minor one — to whoever assesses you. It may be more relevant to the current presentation than it seems.
Take the Next Step
Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
Frequently Asked Questions
Further reading
Related reading
Shoulder pain is rarely just a local problem — scapular position, thoracic kyphosis and the surrounding myofascial system all influence how load is shared across the shoulder girdle, including the AC joint. This pillar article explains the fascial lens we bring to shoulder presentations.
Read Article →Rotator cuff tendinopathy is the most common cause of the shoulder's mid-range painful arc — a different presentation to AC joint end-range pain but one that can overlap. If you're not certain which pattern fits, this page explains the rotator cuff presentation and how we differentiate the two.
Read More →References
- PubMed Hind J, Sidhu GAS, Arealis G, Khadabadi NA, Ashwood N (2022). An algorithmic approach to shoulder pathology. Journal of Family Medicine and Primary Care, 11(9), 5510–5515.
- PubMed Pastor MF, Averbeck AK, Welke B, Smith T, Claassen L, Wellmann M (2016). The biomechanical influence of the deltotrapezoid fascia on horizontal and vertical acromioclavicular joint stability. Archives of Orthopaedic and Trauma Surgery, 136(4), 513–519.
- PubMed Czerwonatis S, Dehghani F, Steinke H, Hepp P, Bechmann I (2020). Nameless in anatomy, but famous among surgeons: the so called "deltotrapezoid fascia". Annals of Anatomy, 231, 151488.
- PubMed Hawthorne BC, Mancini MR, Wellington IJ, DiCosmo MB, Shuman ME, Trudeau MT, et al. (2023). Deltotrapezial stabilization of acromioclavicular joint rotational stability: a biomechanical evaluation. Orthopaedic Journal of Sports Medicine, 11(1), 23259671221119542.
- PubMed Schöbel T, Wendler T, Heilmann R, Fischer J-P, Schleifenbaum S, Theopold J, Hepp P (2025). The deltotrapezial fascia stabilizes the AC-joint and its reconstruction restores the horizontal stability in AC-joint separations: a biomechanical comparison. Journal of Shoulder and Elbow Surgery, 34, 928–936.
- PubMed LeVasseur MR, Mancini MR, Kakazu R, et al. (2022). Three-dimensional footprint mapping of the deltoid and trapezius: anatomic pearls for acromioclavicular joint reconstruction. Arthroscopy, 38(3), 701–708.
- PubMed Carvalhais VOC, Ocarino JM, Araújo VL, Souza TR, Silva PLP, Fonseca ST (2013). Myofascial force transmission between the latissimus dorsi and gluteus maximus muscles: an in vivo experiment. Journal of Biomechanics, 46(5), 1003–1007.
- PubMed Vleeming A, Pool-Goudzwaard AL, Stoeckart R, van Wingerden JP, Snijders CJ (1995). The posterior layer of the thoracolumbar fascia: its function in load transfer from spine to legs. Spine, 20(7), 753–758.
- PubMed De Maeseneer M, Forsyth R, Provyn S, et al. (2019). MR Imaging-Anatomical-Histological Evaluation of the Abdominal Muscles, Aponeurosis, and Adductor Tendon Insertions on the Pubic Symphysis: a Cadaver Study. European Journal of Radiology.
- PubMed Ahmadi M, Minoonejad H, Seidi F, Rajabi R, Farhadian M (2025). Effect of anterior oblique sling training program on pain and functional performance of soccer players with chronic groin pain. Anesthesiology and Pain Medicine, 15(1), e148654.
- PubMed Hislop P, Sakata K, Ackland DC, Gotmaker R, Evans MC (2019). Acromioclavicular joint stabilization: a biomechanical study of bidirectional stability and strength. Orthopaedic Journal of Sports Medicine, 7(4), 2325967119836751.
- PubMed Perry NPJ, Omonullaeva NK, Bacevich BM, Nascimento RJ, O'Donnell EA, Price MD, Mazzocca AD (2023). Acromioclavicular joint anatomy and biomechanics: the significance of posterior rotational and translational stability. Clinics in Sports Medicine, 42(4), 557–571.