Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
📄 Free 2-Week Rehab Program — request your copy
What Is Rotator Cuff Tendinopathy?
The rotator cuff is a group of four muscles that surround the shoulder joint — supraspinatus, infraspinatus, subscapularis, and teres minor. Together, they stabilise the ball of the humerus in the socket (glenoid) and control rotation of the arm. Without them working in a coordinated way, the shoulder cannot function properly.
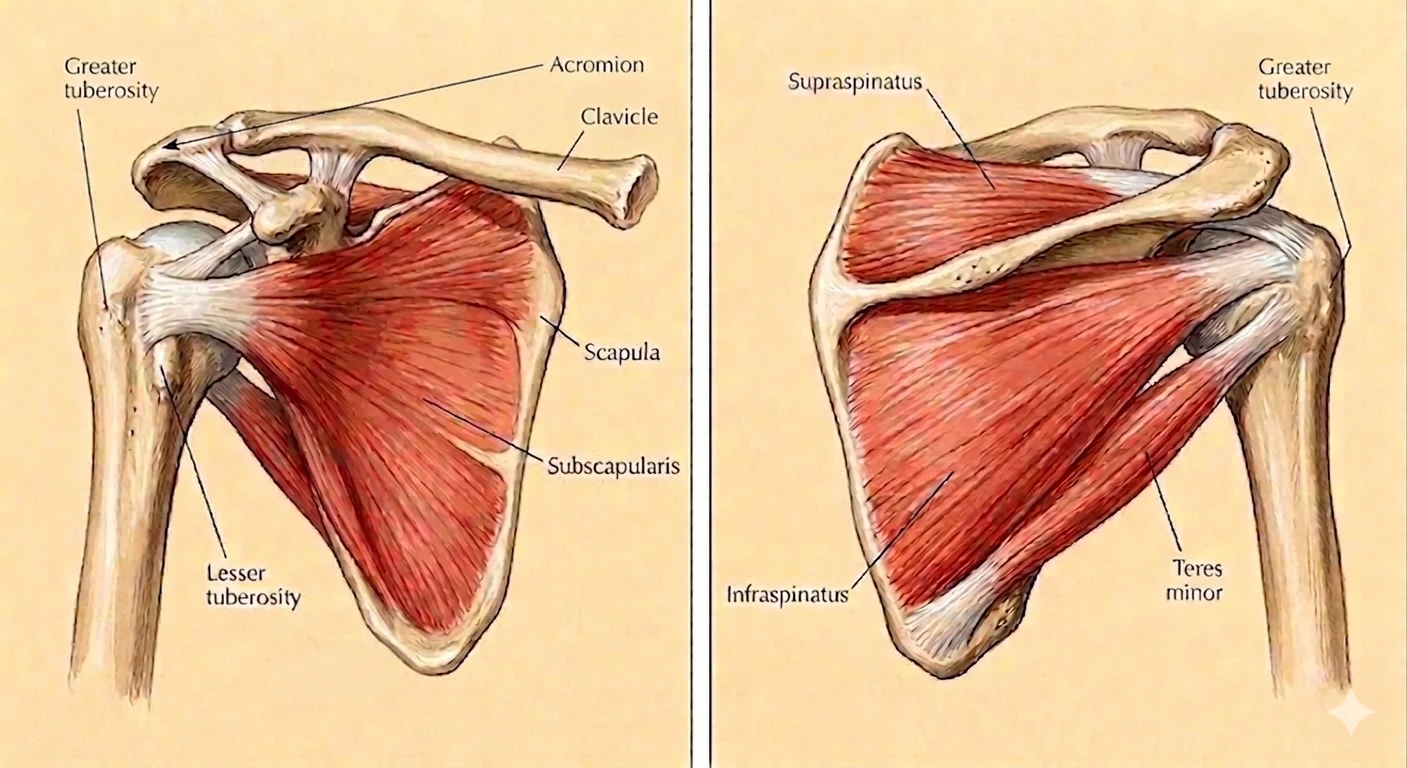
Tendinopathy refers to a change in the internal structure of the tendon — it is distinct from acute inflammation and is better understood as a continuum of tissue response to load. The supraspinatus is the most commonly affected tendon, though infraspinatus and subscapularis involvement is frequently seen in clinical practice as well.
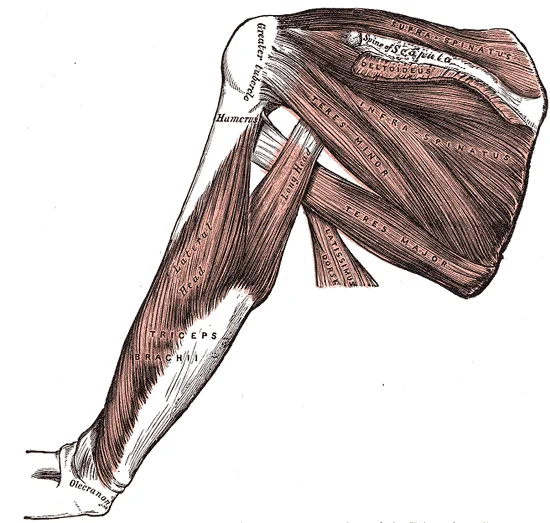
Posterior view of the shoulder — three of the four rotator cuff muscles visible from behind: supraspinatus (superior), infraspinatus (middle), and teres minor (inferior). All three insert onto the posterior facets of the greater tuberosity of the humerus. Together with subscapularis anteriorly, they centre the humeral head on the glenoid during arm movement — and it is their tendons' inability to adequately perform this centring role that underlies most subacromial loading problems. Illustration: Henry Vandyke Carter, Gray's Anatomy (1918) — public domain.
| Feature | Detail |
|---|---|
| Most commonly affected | Supraspinatus tendon (insertion at greater tuberosity) |
| Also frequently involved | Infraspinatus, subscapularis |
| Typical location of pain | Anterior and lateral shoulder; may radiate into the upper arm |
| Characteristic finding | Painful arc of movement (approximately 60–120° of abduction) |
| Night symptoms | Common — particularly lying on the affected side |
| Weakness | Resisted abduction, external rotation, or internal rotation depending on which tendon is involved |
| Age of common presentation | Late 30s and beyond, though younger athletes are commonly affected |
The research describes rotator cuff pathology as a continuum — from early reactive change through tendon dysrepair and, at the far end, to degenerative pathology. Where on that continuum a person sits has significant implications for how load should be managed, which is one reason a thorough assessment matters.

The supraspinatus tendon passes through the subacromial outlet on its way to the greater tuberosity. The width of this space is dynamic — scapular position, thoracic mobility, and rotator cuff tone all influence it.
Who Typically Experiences This?
Overhead workers and tradespeople
Painters, electricians, tilers, and others whose work keeps their arms elevated for sustained periods place consistent compressive and tensile load through the supraspinatus tendon. When the shoulder's kinetic chain is less than optimal — tight thoracic spine, restricted hip rotation, reduced trunk stability — that load concentrates at the tendon rather than being distributed across the system. In our clinical experience, this group often presents having developed symptoms gradually, with a long history of "managing through it" before the tendon can no longer adapt.
Gym athletes and overhead lifters
Pull-ups, overhead pressing, bench press, Olympic lifting — these movements demand precise shoulder mechanics to keep compressive and shear forces within the tendon's capacity. When scapular positioning is altered, when thoracic rotation is limited, or when load has been progressed faster than the tendon can adapt, tendinopathy frequently results. This is particularly common around periods of training intensification. The frustrating reality for this group is that the tendon does not respond well to complete rest — deloading, not stopping entirely, is usually the more productive path.
Desk workers and people with sustained posture patterns
Sustained sitting posture — particularly with a rounded upper back and protracted shoulders — creates a specific mechanical loading pattern at the shoulder. The scapula sits in a position that reduces the outlet space above the supraspinatus, and the muscles of the posterior rotator cuff are chronically lengthened and under-recruited. Over time, the tendon is asked to do more stabilising work with less support from the broader kinetic chain. We commonly see this group presenting with a combination of shoulder and neck symptoms.
Masters and recreational athletes
Swimming, tennis, golf, and recreational sports all generate significant rotator cuff demand through repetitive overhead or rotational movement. In this group, age-related changes to tendon biology mean the tendon's ability to adapt to load is reduced, and recovery from loading episodes is slower. The key, again, is load management — not avoidance.
The person who "just reached for something"
This presentation — acute onset from a trivial movement — almost always reflects a tendon that was already approaching its load capacity. The reach was the final increment, not the cause. This is an important distinction clinically, because it reframes the question from "what happened to my shoulder?" to "what has been building up over time?"
The Fascial Lens: Why We See This Differently
The rotator cuff tendons sit within a broader fascial and kinetic chain system. How load reaches the shoulder — and how well it is distributed once it gets there — depends on everything upstream and downstream of the joint.
The kinetic chain and the shoulder
Force generated by the lower limb and trunk is transmitted upward through the thoracolumbar fascia, the thoracic spine, the scapular stabilisers, and into the glenohumeral joint. When any link in that chain is restricted — hip mobility, trunk rotation, thoracic extension, scapular upward rotation — the shoulder must compensate. The rotator cuff absorbs load that should have been shared more broadly. Over time, this concentrated loading drives tendinopathic change.
Research on overhead throwing athletes has demonstrated this well: kinetic chain deficits at the hip, core, and thoracic spine are consistently associated with increased shoulder injury risk [122]. What holds for throwing athletes holds, in principle, for anyone performing repeated overhead work.
Scapular mechanics and the supraspinatus outlet
The supraspinatus passes through a narrow anatomical corridor between the top of the humerus and the underside of the acromion. The width of that space is not fixed — it changes with scapular position. When the scapula rotates upward and tilts posteriorly as the arm lifts, the space opens appropriately and the supraspinatus passes through without mechanical interference. When this scapular motion is reduced or poorly timed, the space narrows, and the tendon (and the bursa immediately above it) is compressed with every overhead movement.
In our assessment, scapular motor control is always evaluated in shoulder presentations — not as a box-ticking exercise, but because what we find there directly informs how we approach rehabilitation.
The fascial envelope of the shoulder
The rotator cuff muscles are enveloped in deep fascia that connects continuity with the cervical and thoracic regions. Fascial densification — a reversible increase in the viscosity of the loose connective tissue between fascial layers — can alter the normal gliding movement of tissue planes and change how force is transmitted to the tendons. In a cadaveric study documenting the anatomy of the posterior shoulder and upper limb fascial system, Stecco and colleagues identified continuous fascial paths linking the posterior shoulder and brachial regions, providing an anatomical basis for why restricted tissue planes in the neck and upper thorax can contribute to shoulder loading patterns [115].
Why the tendon is often the last thing to treat
This is the core of our clinical perspective. Tendon rehabilitation matters — progressive loading is the backbone of tendinopathy management. But unless the mechanical environment that overloaded the tendon is also addressed, the load problem remains. We aim to resolve both: restore fascial mobility and kinetic chain function, then progressively reload the tendon in a better mechanical environment.
What Does the Research Say?
The continuum model of tendinopathy
A widely-cited framework describes rotator cuff pathology as a spectrum rather than a fixed diagnosis. Early-stage reactive tendinopathy — a short-term cellular response to overload — is potentially fully reversible with appropriate load management. Mid-stage tendon dysrepair involves more structural disorganisation but remains modifiable. Late-stage degenerative change reflects more significant structural disruption. The clinical implication is that stage matters: the optimal management strategy differs significantly depending on where on that spectrum the person presents [116].
The 2025 Clinical Practice Guideline for Rotator Cuff Tendinopathy
A 2025 multidisciplinary clinical practice guideline recommends exercise therapy — particularly progressive loading — as the primary intervention for RC tendinopathy. Manual therapy is recommended as an adjunct to exercise, not as a standalone treatment. The guideline emphasises matching load to the tendon's current capacity and progressing systematically rather than avoiding load altogether [117].
Fascial manipulation for chronic shoulder pain
A pilot study applied fascial manipulation to 28 subjects with chronic posterior shoulder and brachial pain using a specific sequence of treatment centres identified through cadaveric dissection. Three sessions over approximately four weeks produced a mean 57% reduction in pain on a visual analogue scale (from 77mm to 32.8mm, p<0.0001), with benefit maintained at three-month follow-up [115].
Fascial manipulation across musculoskeletal conditions
A systematic review of fascial manipulation for musculoskeletal pain and disability found consistent positive effects across multiple body regions. The authors noted that the FM method demonstrated significant pain reduction and functional improvement compared to control conditions in the studies reviewed [19].
Fascia in sports medicine — the consensus position
A consensus statement from sports medicine researchers concluded that fascial tissue plays a critical role in force transmission, proprioception, and injury recovery — and that targeted manual therapy and loading strategies directed at fascial health are warranted in musculoskeletal rehabilitation [106].
How We Approach Rotator Cuff Tendinopathy
Our assessment begins with a detailed clinical history — understanding when symptoms started, what aggravates and eases them, what loading history looks like, and what has been tried before. This is followed by a movement assessment and manual palpatory examination.
Fascial Manipulation assessment
We assess the fascial system of the shoulder, upper limb, neck, and thoracic regions systematically. Using the Stecco FM approach, we identify centres of coordination (CCs) — points along the deep fascia where palpatory findings suggest densification. Treatment is applied to these points via precise deep friction, aiming to restore fascial gliding and normal force distribution to the shoulder.
Movement rehabilitation
Once fascial mobility is addressed, we direct attention to the movement patterns that were loading the tendon. This typically involves scapular motor control, thoracic mobility, and progressive rotator cuff loading — starting with isometric holds and progressing toward the functional demands of the person's sport or occupation.
Load management
The tendon requires load to recover and adapt — but the type and amount of load matters. We collaborate with you on a loading strategy that keeps the tendon in its adaptive window: enough to stimulate tendon remodelling, not so much that it drives reactive flare.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Keep the tendon loaded — but appropriately
Rotator cuff tendons do not recover well with complete rest. Gentle, pain-free movement — below the threshold that provokes significant pain — helps maintain tendon health and prevents the deconditioning that makes return to activity harder. The goal is to find the level of load the tendon can currently tolerate, not to stop using the shoulder entirely.
2. Work on your thoracic spine
Most people with shoulder tendinopathy have significant restriction in thoracic extension and rotation. A simple daily practice of thoracic extension over a rolled towel or foam roller — aiming for ten repetitions morning and evening — can make a meaningful difference to how the shoulder moves and how much load reaches the tendon.
3. Assess your sleep position
Lying directly on the affected shoulder compresses the supraspinatus against the acromion for hours at a time. If night pain is significant, experimenting with lying on the unaffected side with a pillow supporting the top arm in a neutral position can reduce symptom disruption substantially.
4. Don't reach overhead with a protracted shoulder
The position that most consistently irritates RC tendinopathy is reaching overhead with the shoulder rolled forward and the thoracic spine in flexion. If you need to reach overhead repeatedly, consciously drawing the shoulder blade back and down before lifting — and extending slightly through the upper back — reduces the compressive load on the tendon considerably.
Take the Next Step
Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
📄 Free 2-Week Rehab Program — request your copy
Frequently Asked Questions
Further reading
Related reading
Rotator cuff tendinopathy is shaped by the mechanical environment around the shoulder — scapular position, thoracic mobility, and the posterior chain all influence how compressive load is distributed at the supraspinatus. This pillar article explains the fascial framework governing shoulder mechanics.
Read Article →AC joint pain and rotator cuff tendinopathy are the two most common causes of shoulder pain in active adults. They share overlapping anatomy but produce pain in a characteristically different part of the range — end-range versus mid-range. This page explains the distinguishing features and how we assess each.
Read More →References
- PubMed Lewis JS (2009). Rotator cuff tendinopathy: a model for the continuum of pathology and related management. British Journal of Sports Medicine, 43(9), 649–660.
- PubMed Desmeules F, Roy JS, Lafrance S, et al. (2025). Rotator Cuff Tendinopathy Diagnosis, Non-Surgical Medical Care and Rehabilitation: A Clinical Practice Guideline. Journal of Orthopaedic & Sports Physical Therapy. Advance publication.
- PubMed Day JA, Stecco C, Stecco A (2009). Application of Fascial Manipulation© technique in chronic shoulder pain — anatomical basis and clinical implications. Journal of Bodywork and Movement Therapies, 13(2), 128–135.
- PubMed Arumugam A, et al. (2021). Effectiveness of fascial manipulation on pain and disability in musculoskeletal conditions: a systematic review. Journal of Bodywork and Movement Therapies, 25, 100–109.
- PubMed Chu SK, Press JM (2016). The kinetic chain revisited: new concepts on throwing mechanics and injury. PM&R, 8(3 Suppl), S69–S77.
- PubMed Wilke J, et al. (2018). Not merely a protective packing organ: a review of fascia and its force transmission capacity. Journal of Applied Physiology, 124(1), 234–244.
- PubMed Zügel M, Maganaris CN, Wilke J, et al. (2018). Fascial tissue research in sports medicine: from molecules to tissue adaptation, injury and diagnostics — consensus statement. British Journal of Sports Medicine, 52(19), 1247.