Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Is De Quervain's Tenosynovitis?
De Quervain's tenosynovitis (DQT) is a stenosing condition of the first dorsal compartment of the wrist, affecting the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons. These two tendons run side by side through a fibro-osseous tunnel on the radial side of the wrist, covered by the extensor retinaculum — a thick fascial band that holds the extensor tendons in place across the back of the wrist.
When the gliding mechanism between the tendons and the retinaculum is disrupted — through repetitive loading, sustained thumb-abduction positions, or direct mechanical overload — the tendons and their surrounding sheath thicken. The tunnel becomes relatively too small for its contents, causing pain, swelling, and a characteristic catching sensation with thumb movement.
| Feature | Detail |
|---|---|
| Tendons affected | Abductor pollicis longus (APL) and extensor pollicis brevis (EPB) |
| Key fascial structure | First dorsal compartment of the extensor retinaculum |
| Symptom location | Radial styloid and base of thumb; may radiate proximally into forearm or distally into thumb |
| Provocation | Lifting with extended thumb, pinching, wrist ulnar deviation with thumb tucked (Finkelstein test) |
| Population | Predominantly women 30–50; new parents; manual workers; racquet and grip-sport athletes |
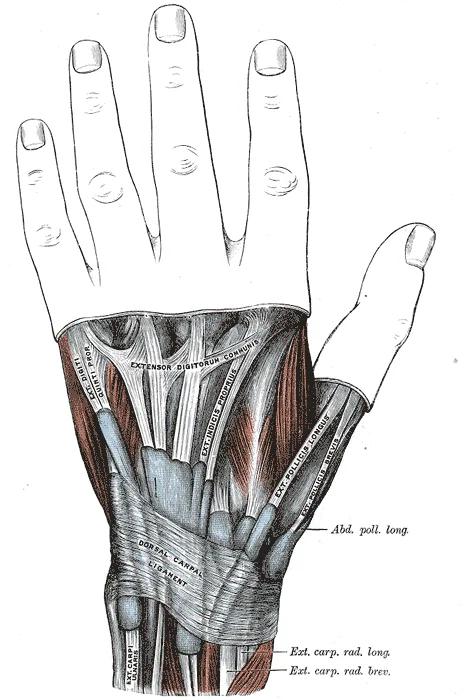
The abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons passing through the first dorsal compartment at the radial styloid — the site of De Quervain's tenosynovitis. Both tendons share a common fibrous sheath as they pass under the extensor retinaculum; repetitive thumb and wrist loading causes friction and thickening of this sheath, compressing the tendons within it. The characteristic pain of De Quervain's is reproduced by stretching these tendons — the basis of the Finkelstein test. Illustration: Henry Vandyke Carter, Gray's Anatomy (1918) — public domain.
Who Typically Experiences This?
New and Recent Parents
Lifting and supporting an infant requires sustained thumb abduction and wrist loading — precisely the movement pattern that loads the APL and EPB. New parents commonly develop DQT within weeks of a baby arriving, often bilaterally. The combination of repetitive load, sleep deprivation, and reduced recovery time creates a tissue environment where cumulative stress exceeds capacity. This is one of the most common presentations of DQT in clinical practice.
Desk Workers with Heavy Mouse or Trackpad Use
Sustained radial deviation and pinch grip at the keyboard and trackpad loads the first dorsal compartment repeatedly throughout the working day. This population often presents more insidiously — symptoms build over weeks rather than appearing with a specific incident — and are often attributed initially to "wrist strain" or repetitive stress.
Olympic Weightlifters and Barbell Athletes
Hook grip (used in Olympic lifting) places the thumb in sustained flexion under high load, and the transition from hook grip to receiving positions creates repeated APL and EPB loading. Front rack and overhead positions with wrist extension load the first compartment differently but can also contribute. In this population, DQT often correlates with spikes in training volume or load rather than absolute training intensity.
Racquet Sport and Grip Athletes
Backhand strokes in tennis and padel, and the wrist snap in badminton and squash, generate repetitive radial deviation under load. This is a well-documented mechanism for first dorsal compartment overload. Athletes in these sports are often high-frequency trainers, and load management is a central part of managing this condition.
The Fascial Lens: Why We See This Differently
The extensor retinaculum is not a passive strap. It is a fascial structure — a dense, organised arrangement of connective tissue — continuous with the dorsal forearm fascia proximally and with the dorsal hand fascia distally. The tendons of the extensor compartments do not glide through bony grooves alone; they glide within a fascial system, and the quality of that gliding depends on the health of the loose connective tissue layer — the paratenon — between tendon and retinaculum.
In the Stecco model of fascial anatomy, this loose connective tissue layer is where densification occurs. Increased hyaluronan viscosity in this layer reduces the ability of adjacent layers to slide relative to each other. In the first dorsal compartment, this means the APL and EPB tendons lose their ability to glide freely under the retinaculum, producing the friction-like loading that drives tissue thickening and pain.
This is why the retinaculum is central to both the conservative and surgical management of DQT. Surgically, the retinaculum is released to widen the tunnel. Conservatively — and from a fascial perspective — the aim is to restore gliding within the first compartment and to address the forearm fascial environment that contributes to first-compartment loading.
The forearm extensor chain is relevant here. The APL and EPB originate from the posterior forearm and interosseous membrane. Their fascial environment includes the entire dorsal forearm compartment. Restriction anywhere along the extensor chain — from the lateral epicondyle and common extensor origin to the extensor retinaculum — can influence loading at the first compartment. We view the first dorsal compartment as the distal end of this chain, not an isolated anatomical unit.
The tendinopathy continuum model is also directly applicable. Early DQT is a reactive tendinopathy — load exceeds capacity, the tendon and sheath respond with rapid cellular activity. At this stage, load management is the priority. In more persistent presentations, there is a degree of tendon disrepair that requires graduated reloading alongside any tissue work. The approach differs depending on where on the continuum the presentation sits. [1]
What Does the Research Say?
Corticosteroid injection with thumb spica immobilisation has the strongest current evidence for pain reduction in de Quervain's tenosynovitis. A 2023 systematic review and network meta-analysis (Challoumas et al.) analysed 30 randomised controlled trials involving 1,663 patients and found that local corticosteroid injection combined with thumb spica immobilisation for 3–4 weeks produced significant improvements in pain and function compared with other treatments. Ultrasound-guided injection was superior to conventional injection for pain reduction. [2]
What this means for our approach: The evidence clearly supports corticosteroid injection as a first-line option for pain management in DQT, and we will say so honestly. Our clinical role is to assess and address the mechanical loading environment — the fascial environment of the first dorsal compartment, the forearm extensor chain, and the movement patterns that continue to load the structure — in conjunction with, or following, any medical management. Injection addresses the local inflammatory response; it does not address the loading context that produced it.
Load management principles from tendinopathy research inform our approach to graduated return to activity. The tendinopathy continuum model (Cook & Purdam, 2009) provides a framework for understanding the stage of the condition and guiding load management accordingly. [1]
How We Approach De Quervain's Tenosynovitis
Our assessment examines the first dorsal compartment directly — palpation of the APL and EPB tendons, the retinaculum, and the paratenon environment — alongside assessment of the dorsal forearm fascial chain and movement patterns that load the first compartment.
We assess:
- The quality of tendon gliding under the retinaculum
- Fascial restriction along the dorsal forearm extensor chain
- Wrist and thumb position under load (grip strategy, lifting mechanics)
- Frequency and volume of provocative loading in daily life and training
Where fascial densification is identified along the extensor chain, Fascial Manipulation is directed at the relevant centres of coordination. Movement retraining addresses the wrist and thumb positions that drive cumulative loading on the first compartment. Load management guidance is provided for sport, work, and daily activities.
The goal is to restore the mechanical environment of the first compartment — improving tendon gliding, reducing forearm fascial tension, and modifying the patterns that continue to load the structure.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Use a thumb spica splint for load management.
A thumb spica splint, which holds the wrist and CMC joint of the thumb in a neutral position, reduces loading on the APL and EPB during daily activities. This is supported by the evidence as part of first-line management. Splints are available over the counter at most pharmacies. Wearing one during provocative activities — lifting, carrying, keyboard use — can reduce cumulative load while the tissue recovers.
2. Modify how you lift your baby or carry loads.
Rather than lifting with the thumb abducted and wrist loaded, try scooping with both hands supporting the infant's body weight through the forearm rather than the thumb-wrist lever. This reduces the specific load on the first compartment during what is often the highest-frequency provocative activity.
3. Address your forearm extensor loading.
Gentle forearm extensor stretching — wrist flexed with elbow extended, rotating the forearm into pronation — can help maintain extensibility along the dorsal forearm chain. Avoid aggressive stretching if symptoms are acute; at that stage, load reduction takes priority.
4. Review your grip and wrist position under load.
In gym settings, assess wrist position in pressing movements, carries, and pulling exercises. Small adjustments to grip width or wrist alignment can meaningfully reduce first-compartment loading during training.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
De Quervain’s tenosynovitis is a disorder of the first dorsal compartment — but the fascial environment of the entire forearm and wrist shapes how repetitive load is distributed to the APL and EPB tendons. This pillar article covers the full upper limb fascial context.
Read Article →T1ρ MRI evidence shows that fascial tissue state can be objectively measured and altered — directly relevant to de Quervain’s, where peritendinous fascial densification contributes to the restricted gliding environment around the extensor tendons. This article reviews the structural evidence.
Read Article →References
- PubMed Cook JL, Purdam CR (2009). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6), 409–416.
- PubMed Challoumas D, Ramasubbu R, Rooney E, Seymour-Jackson E, Putti A, Millar NL (2023). Management of de Quervain Tenosynovitis: A Systematic Review and Network Meta-Analysis. JAMA Network Open, 6(10), e2337001.