Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
What Is Trigger Finger?
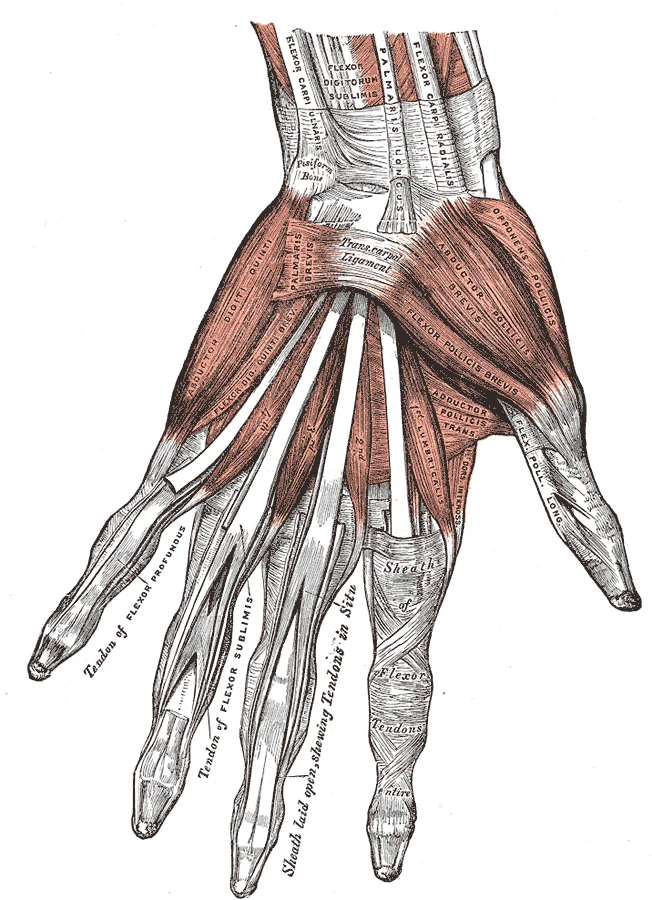
Trigger finger — properly called stenosing tenosynovitis — is a condition where one of the flexor tendons of the hand catches or locks as it attempts to pass through a fibrous ring called the A1 pulley. The A1 pulley is a thickened band of connective tissue that overlies the metacarpophalangeal (MCP) joint at the base of each finger, forming the entrance to the fibro-osseous tunnel through which the flexor tendons travel to the fingertip.
In trigger finger, either the pulley thickens and narrows, or a nodule develops on the tendon itself — or both — creating a mechanical mismatch between the tendon and the tunnel it must pass through. The result is the characteristic triggering: the finger catches in flexion and snaps or locks as the tendon forces its way through.
| Feature | Detail |
|---|---|
| Structure involved | A1 pulley at the MCP joint; flexor digitorum superficialis and profundus tendons |
| Symptom | Finger clicking, catching, or locking in flexion; may be painful or painless |
| Location | Most commonly ring finger, middle finger, and thumb (trigger thumb); any digit can be affected |
| Prevalence | Approximately 2–3% of the general population; significantly higher in diabetics (up to 10%); more common in women aged 40–60 |
| Grading | Grade 1: pain/tenderness; Grade 2: catching, actively correctable; Grade 3: locking, passively correctable; Grade 4: fixed flexion deformity |
Who Typically Experiences This?
Desk Workers and Those with Prolonged Gripping
Sustained grip — keyboard use, mouse work, extended periods of fine motor activity — repetitively loads the flexor tendons against the A1 pulley. Over time, this cumulative loading drives the metaplastic changes at the pulley that narrow the tendon passage. The ring finger and middle finger are most commonly affected in keyboard-heavy workers.
Manual Workers and Tradespeople
Sustained or repetitive grip with tools is the classic occupational mechanism for trigger finger. Carpenters, mechanics, plumbers, and anyone whose work involves sustained hand grip across a day are at elevated risk. The combination of high grip force and prolonged tendon loading is a common mechanism for pulley thickening.
Diabetics
Type 1 and Type 2 diabetes are strongly associated with trigger finger — prevalence estimates in diabetic populations reach 10%, compared with 2–3% in the general population. The mechanism involves glycation of collagen in the pulley and tendon sheath, altering tissue stiffness and gliding capacity. Management in this population requires awareness of the broader connective tissue context.
Gym Athletes and Weightlifters
Barbell pulling movements — deadlifts, rows, cleans, pull-ups — subject the flexor tendons to high-force repetitive loading. Olympic lifting athletes who train with hook grip face particular loading demands on the flexor tendons of the thumb. Volume spikes in grip-intensive training are a common precipitant.
The Fascial Lens: Why We See This Differently
The A1 pulley is not an isolated anatomical structure. It is a fascial condensation — a thickened, organised band of connective tissue that forms the proximal entrance of the flexor tendon sheath. It is continuous with the palmar aponeurosis superficially, which in turn connects to the palmaris longus tendon and the antebrachial fascia of the forearm.
This continuity matters clinically. The palmar aponeurosis is part of the hand's fascial system — a tension-transmitting sheet that distributes grip forces across the palm and connects the forearm flexor compartment to the digits. Loading patterns in the forearm and palm influence the mechanical environment at the A1 pulley. Fascial restriction anywhere along this chain — from the forearm flexors to the palmar fascia — alters how force is distributed to the individual pulleys.
The Stecco model of fascial anatomy describes how densification of the loose connective tissue layer between adjacent fascial layers reduces gliding capacity between them. At the level of the flexor tendon sheath, this densification impairs the ease with which the tendon moves relative to the sheath and pulley — a mechanism directly analogous to what is observed in trigger finger: the tendon and pulley relationship becomes mechanically less favourable as tissue quality deteriorates.
This framing does not suggest that manual therapy reverses a Grade 3 or 4 trigger finger — the structural changes at the pulley at that stage often require injection or surgical release. What it does suggest is that assessing the forearm fascial and loading environment, in early-stage presentations or as part of post-injection rehabilitation, is relevant to understanding why the condition developed and to reducing the mechanical drivers that perpetuate it.
What Does the Research Say?
The evidence base for trigger finger management is strongest for corticosteroid injection and surgical release. Corticosteroid injection into the tendon sheath is effective for Grade 1–3 presentations, with success rates of approximately 60–70% at short-term follow-up, though recurrence rates are significant — particularly in diabetics. Surgical release of the A1 pulley has very high success rates and low complication rates. In clinical practice, the evidence clearly supports these interventions as primary management for moderate-to-severe trigger finger. We acknowledge this honestly.
Conservative management — including splinting, tendon gliding exercises, and manual therapy — is most applicable in early-stage or recurrent presentations. The literature documents positive outcomes from splinting (MCP joint extension splinting), tendon and nerve gliding exercises, and activity modification in Grade 1–2 trigger finger, and as an adjunct following injection or post-surgically. Manual therapy targeting the forearm flexor fascial chain and improving tendon gliding capacity is a clinically reasonable approach in this context, though robust RCT evidence for manual therapy alone as a primary treatment is limited.
Fascial densification can impair tendon gliding independent of structural narrowing. Research into fascial entrapment neuropathy and tendon-sheath mechanics demonstrates that the loose connective tissue layer between the tendon and its sheath plays an important role in gliding quality. When this layer is compromised — through repetitive loading, glycation, or fascial densification — the tendon-sheath interface becomes mechanically less favourable. This model supports a role for soft-tissue assessment of the forearm flexor chain and palmar fascia as part of conservative management and rehabilitation. [1]
How We Approach Trigger Finger
Our assessment examines the A1 pulley and the tendon directly — palpation for nodule formation, pulley thickening, and triggering — alongside the palmar fascia, the forearm flexor compartment, and the grip patterns that continue to load the structure.
In Grade 1–2 presentations, our approach aims to:
- Reduce cumulative loading on the A1 pulley through activity modification and gripping technique changes
- Address fascial restriction along the forearm flexor chain and palmar aponeurosis
- Guide tendon gliding exercises that maintain tendon mobility within the sheath
- Advise on MCP extension splinting where appropriate
For Grade 3–4 presentations, we will recommend co-management with your GP for consideration of corticosteroid injection or surgical referral — these are often the appropriate primary interventions at that stage. We can contribute to rehabilitation following these procedures, with the same goals of restoring the mechanical environment and reducing recurrence risk.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Perform tendon gliding exercises.
Tendon gliding exercises — moving the fingers through a series of specific positions (straight, hook fist, full fist, tabletop) — aim to maintain the full excursion of the flexor tendons through the pulley system. These reduce stiffness and maintain gliding capacity. They are most effective in Grade 1–2 presentations and post-injection rehabilitation. A practitioner can demonstrate the specific technique for your presentation.
2. Modify your grip patterns.
Avoid sustained grip in a fully flexed position where possible. Take regular breaks from sustained gripping activities. Consider using padded or larger-diameter handles on tools and equipment to reduce peak force at the pulley. In gym settings, using straps for heavy pulling movements can reduce flexor tendon loading.
3. Consider MCP extension splinting at night.
Splinting the MCP joint in neutral or slight extension during sleep prevents the finger from locking in flexion overnight and reduces the risk of Grade 3+ progression. Over-the-counter trigger finger splints are available; a hand therapist or practitioner can advise on the appropriate fit and wearing schedule.
4. If you have diabetes, seek early assessment.
Trigger finger in diabetic patients tends to progress more rapidly and respond less predictably to conservative management. Early assessment — including consideration of injection timing relative to glucose management — is recommended. This is not something to monitor-and-wait with in this population.
Take the Next Step
Ready to get on top of this?
Call Now — speak with our team
Book Online — available 24/7
Frequently Asked Questions
Further reading
Related articles from the blog
Trigger finger develops when the flexor tendon can no longer glide freely through the A1 pulley — a problem rooted in the fascial and tenosynovial environment of the palm and forearm. This pillar article maps the full upper limb fascial context relevant to tendon gliding disorders.
Read Article →T1ρ MRI provides objective evidence that fascial tissue state can be measured and changed — directly relevant to trigger finger, where densification of the peritendinous sheath and palmar fascia restricts tendon excursion. This article reviews the structural findings from Menon 2020.
Read Article →References
- PubMed Stecco C (2019). Fascial entrapment neuropathy. Clinical Anatomy, 32(7), 884–891.